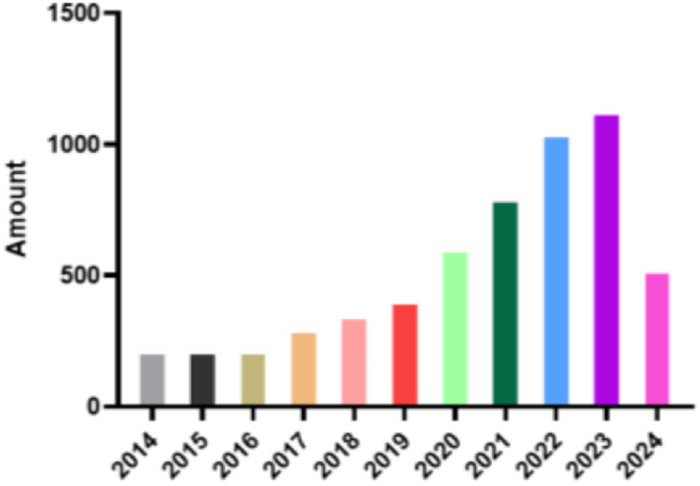
Figure 1.
Number of publications on biomedical materials and pulmonary disease therapy in Web of Science from 2014 to Sep. 2024.
Applications and challenges of biomedical polymer materials in pulmonary diseases
Dayang Xie , Qiannan Cao , Huapan Fang , Yanhui Li , Huayu Tian

Pulmonary diseases including lung cancer [1], pulmonary fibrosis [2], chronic obstructive pulmonary disease (COPD) [3], tuberculosis [4], and asthma [5] are increasingly threatening people's health and lives. With the continuous development of life medicine and pathology, the etiology of lung diseases is gradually being elucidated. Generally, due to the uniqueness of the lung organs, lung diseases are often accompanied by a certain degree of infectivity [6]. The outbreak of novel coronavirus pneumonia coronavirus disease 2019 (COVID-19) occurred globally in 2019, and by the end of 2022, it had infected over 600 million people and caused 6 million deaths. Even after recovery, COVID-19 patients may experience various sequelae, including pulmonary fibrosis and airway lesions [7-9].
Traditional methods of treating pulmonary diseases include surgery, drug therapy, and radiotherapy [10]. Surgical procedures can effectively remove lung lesions but often result in large incisions, slow postoperative healing, and the risk of infection [11]. Drug therapy whether administered intravenously or by inhalation, may have poor targeting due to the complicated physiological environment in the body, leading to damage to normal cells while clearing diseased cells [12,13]. In addition, the cost of radiotherapy is high and radiotherapy can cause serious side effects, such as nausea, vomiting, hair loss, and damage to the immune system [14]. Therefore, there is an urgent need to develop a safe and effective strategy for treating pulmonary diseases. In recent years, with the continuous development of biomedical polymer materials, the application of biomedical polymer materials as a therapeutic strategy in lung diseases has achieved many results, and the number of research results on the science citation index (SCI) has also increased year by year (Fig. 1).
Biomedical polymer materials, with their excellent biocompatibility, tissue targeting, and controllable modification [15-17], have attracted widespread attention from researchers in the field of pulmonary diseases therapy. In general, biomedical polymer materials can effectively encapsulate small molecule drugs, proteins and functional nucleic acids through surface modification [18], efficiently reach lung lesions, and achieve precise treatment of pulmonary diseases [19]. Biopolymeric materials not only play a crucial role in pulmonary drug delivery but are also widely used as scaffold materials in tissue engineering and regenerative medicine to promote cell adhesion, proliferation, and differentiation, thereby repairing or replacing damaged tissues. For instance, nickel-titanium alloy metal scaffolds exhibit excellent flexibility, support performance, and shape memory effects, enabling them to return to their original shape at body temperature, tightly conforming to airway walls and providing stable support [20]. Bai et al. synthesized a photocurable hydrophilic copolymer (PMHB) via free radical polymerization, which serves as a coating material for catheter surfaces with lubricating and antifouling properties [21]. In the field of diagnostics, polymethyl methacrylate (PMMA) can be used to fabricate polymeric biochips for capturing tumor cells, enhancing detection sensitivity and specific capture [22].
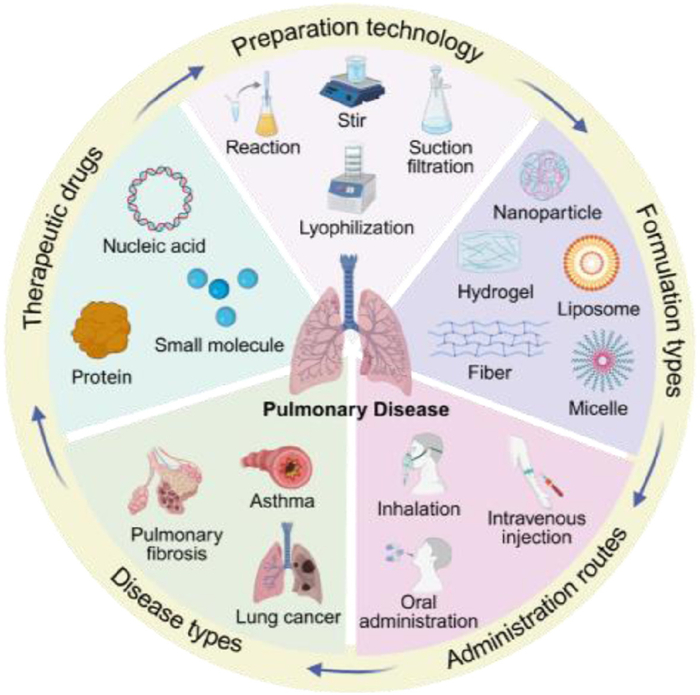
In this review, we mainly discusses the physiological structure of the lungs, the causes and pathological changes of lung diseases, in order to explore the biomedical polymer-based drug-delivery strategies for the treatment of lung diseases. In particular, we systematically introduce the types of biomedical polymer materials, the common types and pathogenesis of pulmonary diseases, traditional treatment methods, and the application of biomedical polymer materials in the treatment of pulmonary diseases (Fig. 2). Moreover, the challenges and opportunities faced by biomedical polymer materials in the field of lung disease therapy are discussed in details and some suggestions are provided for the future application of biomedical polymer materials-mediated pulmonary disease therapy. This article provides useful guidance for the treatment of pulmonary diseases mediated by biomedical polymer materials.
As the respiratory organ within the human body, the lung consists of terminal airways, alveoli, and pulmonary interstitial tissues, and can be further categorized into two principal areas: The conducting airway region and the respiratory region [23]. The structural configuration of the lung dictates its ventilatory function [24]. The conducting airways encompass the nose, pharynx, larynx, trachea, bronchi, bronchioles, and terminal bronchioles [25]. The respiratory region comprises respiratory bronchioles, alveolar ducts, and alveolar sacs [26]. Connective tissue interstitial exists between the bronchi and alveoli, within which lymphatic vessels, nerves, and blood vessels are distributed, along with macrophages, fibroblasts, and other immune cells [27].
The lung serves as the primary site for gas exchange in the human body. It harbors an extensive number of alveoli. The total number of alveoli in an adult ranges from approximately 300–400 million, with the total alveolar area reaching 70–100 square meters [28]. Such an expansive surface area enables the lung to effectuate efficient exchange of oxygen and carbon dioxide. However, it simultaneously furnishes a vast attachment and invasion space for pathogens and tumor cells. The alveolar wall is characterized by its thinness, being composed of a monolayer of epithelial cells. This structure facilitates rapid gas diffusion [29]. Nevertheless, it also renders the alveoli susceptible to incursions by external pathogens. When pathogens are inhaled by the human body, they deposit on the airway and alveolar surfaces within the lungs. In the event that the respiratory defense mechanisms, such as the mucociliary clearance system and alveolar macrophages, fail to promptly and effectively eliminate these pathogens, pulmonary infections are prone to occur [30]. Pulmonary infections result in varying degrees of lung injury. Inflammation represents the primary defensive response to pathogen-induced tissue damage. The general process of inflammation encompasses degeneration, exudation, and proliferation, corresponding respectively to the initiation, tissue damage, and repair phases of inflammation, involving alterations in multiple cellular pathways and signal transduction processes [31,32]. However, uncontrolled activation of cells and the release of cytokines and chemokines may precipitate a lethal "cytokine storm", thereby causing damage to tissues and cells. In severe cases, this can lead to fatal symptoms including lung failure, acute respiratory distress syndrome, and even respiratory failure [33].
Furthermore, the lung is endowed with an extremely rich blood circulation system [34]. The pulmonary artery conveys venous blood from the right ventricle to the lungs. Subsequently, following gas exchange, the pulmonary vein transports oxygen-rich blood back to the left atrium. The abundant blood supply provides ample oxygen and nutrients to the lung tissue, thereby maintaining its normal physiological functions. On the other hand, this also offers favorable conditions for tumor metastasis. Tumor cells can reach the lungs through the bloodstream and then lodge and proliferate within the microvascular bed of the lungs [35]. Moreover, immune cells within the blood may experience "immune overload" when confronted with a large influx of pathogens or tumor cells, thereby resulting in a decline in defensive capabilities [36]. Research indicates that approximately 30%–40% of patients with solid tumors develop lung metastases [37]. This is primarily because the lungs constitute an important hub within the blood circulation and lymphatic circulation systems, providing convenient transportation conditions for tumor cell metastasis [38].
Pulmonary drug delivery represents a highly promising drug-delivery route, particularly for drugs that are prone to hepatic metabolism after therapeutic surgery [39]. Additionally, local drug delivery constitutes a direct approach for achieving enhanced drug accumulation within the lungs, which may be beneficial for the treatment of lung diseases. However, the natural barriers within the lungs cause drug molecules or particles, after inhalation, to become entrapped within the mucus layer [40]. The mucus barrier impacts drug dissolution, impedes the fusion of drugs with epithelial cells, and inhibits the interaction of drugs with cell surfaces and receptors. Overcoming the mucus layer to reach the alveolar epithelial layer remains a crucial biological barrier for effective drug delivery. The pulmonary mucus layer is secreted by goblet cells and submucosal glands and consists of mucin, water, and surfactants [41]. The negatively charged mucin within the mucus forms a mucin-fiber network structure with a variable porosity ranging from 50 nm to 180 nm on the airway surface, which functions to capture inhaled irritants or drug particles. Generally speaking, nanoparticles with hydrophilic surfaces and electrical neutrality possess superior mucus-layer penetration capabilities [42].
The unique physiological structure and irreplaceable functions of the lungs render them vulnerable to the invasion of pathogenic microorganisms [43], the colonization of metastatic tumor cells, and the release of uncontrollable inflammatory factors, thereby leading to the formation of various diseases, including lung cancer, pulmonary fibrosis, COPD, and asthma.
Biomedical polymer materials refer to polymer materials used in the biomedical field that need to ensure that they do not cause significant rejection or toxic reactions when interacting with the tissues and organs of living organisms. Biomedical polymer materials are mainly used in the manufacture of artificial organs, medical devices, drug delivery systems and tissue engineering [44], due to their biocompatibility, biodegradability and excellent physical and chemical properties. In general, biomedical polymer materials can be divided into natural polymer materials and synthetic polymer materials according to their sources.
Natural polymer materials refer to high-molecular compounds existing in nature, which are synthesized in living organisms or formed through natural processes [45]. Such materials come from a wide range of sources and usually have good biocompatibility and degradability. Collagen is mainly extracted from animal skin, bone and connective tissue [46,47]. As a natural polymer material in daily life, collagen is widely used in skin care products. In acute lung injury or chronic lung disease such as COPD, collagen can be used as a scaffold material to help repair damaged lung tissue [48]. By applying collagen matrix topically, it may help support and promote cell growth and antibacterial properties, which can inhibit the growth of certain pathogenic bacteria, making it a potential application in the treatment of lung infections, such as bacterial pneumonia. Moreover, sodium alginate is a natural polysaccharide extracted from brown algae [49], which can form a gel in the physiological environment, which allows it to be used as a carrier to control the release of drugs, thereby increasing the local concentration of drugs and enhancing the therapeutic effect. In the treatment of bronchitis and asthma, sodium alginate can be used to prepare aerosols or aerosols of respiratory drugs, and its gel formation ability can improve the distribution of drugs in the bronchus, reduce the systemic side effects of drugs, and improve the therapeutic effect [50,51]. In addition, sodium alginate may have anti-inflammatory properties that help reduce the inflammatory response of bronchitis and asthma [52]. There are other natural polymer materials, such as cellulose, gelatin, fibroin protein and hyaluronic acid, which have a wide range of application prospects in medicine, medical treatment, food and other fields [53].
Synthetic polymer materials are those specially designed and synthesized polymer materials used in medical fields and are generally biodegradable. These materials not only have good biocompatibility, mechanical properties and chemical stability, but also meet specific medical needs, such as tissue repair, drug delivery and in vivo implants. Polylactic acid (PLA) is a biodegradable synthetic polymer material widely used in medicine and bioengineering [54]. PLA can be used to manufacture drug delivery systems for lung diseases. By loading drugs in the PLA matrix, sustained or controlled release of drugs can be achieved, and drugs can be delivered directly to the lungs to improve the therapeutic effect [55,56]. The biodegradability of PLA allows the drug delivery system to leave no long-term residue in the body, reducing the risk of long-term use [57]. PMMA is a transparent, hard synthetic polymer material [58], and although PMMA has a wide range of applications in the medical field, such as artificial lenses in eye surgery and dental repair materials, it has relatively few applications in lung diseases. To meet specific medical needs, PMMA microspheres or nanoparticles was designed to encapsulate antibiotics, anti-cancer drugs or anti-inflammatory drugs, and deliver the drugs directly to the lungs by inhalation or injection, achieving the effect of local treatment [59,60].
Compared to natural polymer materials, synthetic polymer materials have better repeatability and are not limited by source or batch [61]. However, synthetic polymer materials may carry the risk of immune rejection in the body [62]. One alternative strategy is to combine a natural polymer material with a synthetic polymer material to reduce the immunogenicity of the materials. This new biomedical material can take full advantage of the advantages of natural polymer materials, while improving with synthetic ingredients to meet specific medical needs. For example, combining natural polysaccharides such as sodium alginate with synthetic polymer carriers to prepare nanodrug delivery systems can significantly improve drug safety and lung delivery efficiency in the treatment of lung cancer and COPD [63,64]. Taking advantage of the excellent biocompatibility of collagen, it is combined with synthetic polymer materials to prepare microspheres, that can be applied in pulmonary drug delivery systems [65].
In the clinical treatment of lung diseases, although modern medicine has made remarkable progress, there are still challenges such as drug resistance, high surgical risk, and large side effects of radiotherapy and chemotherapy. The development of biomedical polymers offers more opportunities for the treatment of pulmonary diseases. For instance, when serving as excipients, they can enhance the stability of drug physical and chemical delivery [66]. Additionally, they can be applied in pulmonary implant stents [67]. Many biomedical polymer materials are designed to be biodegradable and can gradually degrade into non-toxic small molecules in the body, avoiding long-term residue problems. By designing a drug carrier system, these materials can achieve controlled release of drugs, and accurately release drugs to the diseased part of the lung through inhalation or injection [68], to achieve the effect of local treatment. Some biomedical polymer materials can be chemically modified or combined with antibacterial agents to obtain antibacterial and anti-inflammatory properties and reduce the risk of postoperative infection and inflammation, such as polymer materials containing silver nanoparticles can inhibit pathogen growth [69,70]. Biomedical polymer materials show many advantages in the treatment of lung diseases, including excellent biocompatibility, controlled biodegradability, precision drug delivery, tissue repair promotion, antibacterial and anti-inflammatory properties [71]. These advantages make biomedical polymer materials an important tool for the treatment of lung diseases, providing more treatment options and better treatment outcomes.
Lung cancer is a common malignant tumor with the highest morbidity and mortality in the world [72], posing a major threat to people's health and life. In general, lung cancer is caused by a variety of factors, including environmental pollution, unhealthy lifestyle habits such as smoking, and genetic factors [73,74]. There are two main types of lung cancer: small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). SCLC progresses more quickly, but drug treatment is more effective than NSCLC. However, NSCLC, which accounts for the majority of lung cancer cases, has a worse prognosis after treatment than SCLC [75]. Common symptoms in lung cancer patients include persistent cough, sputum production, difficulty breathing, chest pain, and advanced, unexplained weight loss [76].
Treatment options for lung cancer depend on the type of lung cancer, how far it has progressed, and the overall health of the patient. Traditional treatment strategies for lung cancer include surgery, radiation therapy, chemotherapy and targeted therapy [77]. Surgery is mainly used for the treatment of early stage lung cancer and may include lobectomy, segmentectomy, or total pneumonectomy [78], depending on the type and extent of lung cancer, and is usually accompanied by lymph node dissection. Radiation uses high-energy X-rays to kill cancer cells, but may also damage normal lung tissue cells [79]. Chemotherapy is usually administered with intravenous drugs to kill cancer cells and is often used for advanced lung cancer or as an adjunct to surgery to relieve symptoms [80]. Targeted therapy is the treatment of specific molecules or signaling pathways in cancer cells, based on molecular differences between cancer cells and normal cells, interfering with the growth, proliferation and survival of cancer cells [81].
Although these traditional treatments have been able to slow the progression of lung cancer to a certain extent and extend the survival of patients, they also face many challenges. For example, surgery is usually only suitable for early stage lung cancer, and many lung cancer patients are not suitable for surgery due to factors such as age, physical condition, and location of the lesion. In addition, treatments such as chemotherapy and radiation can cause a range of side effects, including nausea, vomiting, fatigue, anemia, and immune system suppression [82]. In addition, targeted therapies often cause cancer cells to develop drug resistance and immune escape mechanisms [83,84]. What is more, cancer cells in patients with advanced lung cancer often metastasize to other organs or tissues, such as the lymph nodes, brain, or bone, posing a major challenge to traditional treatment strategies [85].
Currently, there is a lack of more effective and personalized solutions in traditional lung cancer treatment methods. The development of biomedical polymers brings more possibilities for lung cancer treatment and better prognosis [86]. Generally speaking, biomedical polymer materials can be used as drug delivery carriers to enhance the targeting of drug delivery to the lungs, which can achieve good therapeutic effect while minimizing the impact on other tissues and organs [87]. For example, certain biodegradable polymers can encapsulate anti-cancer drugs and release them in a controlled manner at the tumor site in the lungs [88]. This targeted drug delivery reduces the side effects on normal tissues and increases the concentration of drugs at the tumor site, enhancing the therapeutic effect. Nanoparticles made of biomedical polymers can also be engineered to have specific surface properties that target cancer cells, further improving the specificity and efficacy of drug delivery [89].
Many proteins and peptides, such as antibodies, insulin and vaccines, are widely used in the treatment of lung cancer [90]. Biomedical polymers can be compounded with proteins into nanoparticles, thereby improving the stability and targeting of therapeutic proteins [91], which is of great significance for the treatment of lung cancer. Yadav et al. [92] modified poly(lactic-co-glycolic acid) (PLGA) nanoparticles by RGD to improve the effectiveness of cisplatin in the treatment of lung cancer. PLGA is a versatile and clinically approved polymer used for the preparation of nanoparticles, which is composed of different proportions of lactic acid and glycolic acid monomer units, which is metabolized to eventually produce non-toxic product [93]. RGD-modified PLGA nanoparticles have achieved lower cytotoxicity, negligible damage to lung tissue, low systemic toxicity, and high biocompatibility and safety in lung tissue.
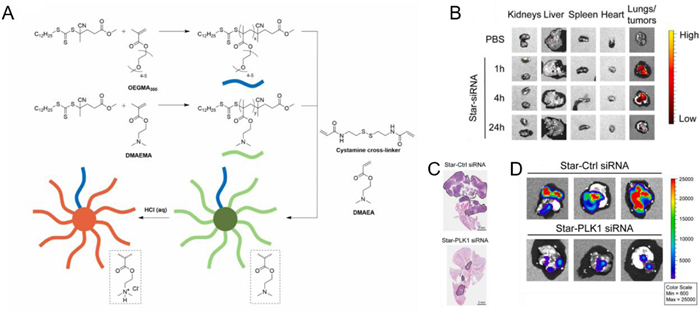
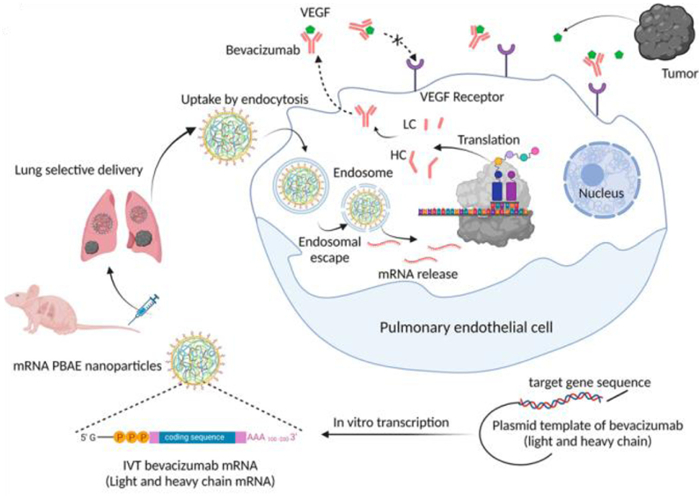
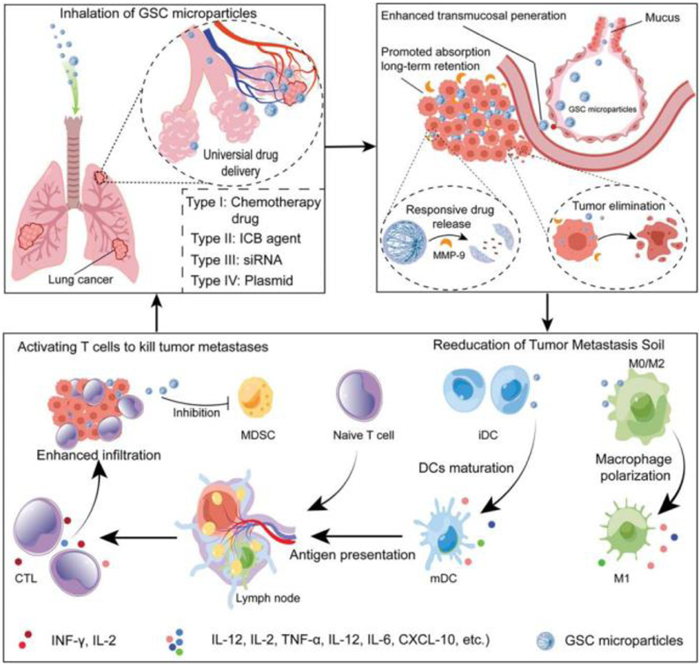
Nucleic acid drugs are nucleic acids themselves or closely related compounds, including natural nucleotides and chemically modified nucleotides, that can be used to treat disease [94-96]. Nucleic acid drugs have the advantages of simple design, short research and development cycle, strong targeting specificity, wide therapeutic fields and long-term performance [97], showing great potential in the treatment of genetic diseases, viral infections, tumors and other fields, and are expected to become the third class of drugs after small molecule drugs and antibody drugs [98]. Ma et al. designed a star polymer-siRNA nanoparticles infused with aerosols to deliver siRNA to the lungs, inhibiting the expression of two genes βⅢ-tubulin and Polo-like kinase 1 (PLK1). slowing the aggressive growth of tumors (Fig. 3A) [99]. The synthesis of core-crosslinked Miktoarm star polymer nanoparticles (star nanoparticles) was achieved through reversible addition-fragmentation chain-transfer (RAFT) polymerization of poly(2-(dimethylamino)ethyl methacrylate) (PDMAEMA) and poly[oligo(ethylene glycol)methyl ether methacrylate] (POEGMA) [100]. Subsequent distribution of biological experiments in mice, in vitro fluorescence imaging of representative organs of mice administered intravenously or by aerosol showed different results, with intravenously administered mice nanoparticles mainly distributed in the kidneys and liver, while aerosol administered mice nanoparticles mostly accumulated in the lungs, and no nanoparticles were found in the kidneys, liver, and spleen at any point in time (Fig. 3B). In an orthotopic mouse lung tumor model, the delivery of siPLK1 using star polymers also achieved very significant therapeutic effects (Fig. 3, Fig. 3). Poly(β-amino esters) (PBAEs) are a class of biodegradable polymers that can be synthesized using various simple chemical methods. The cationic nature of PBAEs enables them to effectively complex with nucleic acids, forming nanoparticles. Additionally, PBAEs exhibit lung-targeting capabilities, making them promising candidates for pulmonary therapies [101]. Le et al. prepared PBAE-lipid nanoparticles by combining PBAEs with dioleoylphosphatidylethanolamine (DOPE) and DMG-PEG in a specific ratio, dissolving the mixture in ethanol. They then vigorously mixed these nanoparticles with mRNA encoding bevacizumab in an acidic aqueous phase, resulting in PBAE lipid nanoparticles containing mRNA. After intravenous administration, these nanoparticles preferentially target the lungs, where they are taken up by pulmonary endothelial cells. Following escape from endosomal-lysosomal compartments, the mRNA is released inside the cells, where it encodes antibodies with bevacizumab functionality, inhibiting the production of vascular endothelial growth factor (VEGF) and consequently suppressing tumor growth (Fig. 4) [102]. Additionally, Rotolo et al. conducted a series of modifications on PBAE, such as multifunctional amines, amino alcohols, and amino thiols. The resulting various polymers were evaluated for mRNA delivery treatment in the lungs, successfully screening out polymers capable of effectively delivering mRNA to the lungs of different animals. This makes future inhalable nucleic acid therapy for lung treatment a possibility [103]. Huang et al. proposed a nanoparticle co-delivery system of gefitinib (Gef) and YAP-siRNA, utilizing block and dendritic polymers, to address the issue of NSCLC resistance to epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKI) (Fig. 5) [104]. These nanoparticles were effectively internalized by NSCLC cells in both CDX and PDX models and were able to escape from lysosomes/endosomes. In the reductive cellular environment, they released Gef and YAP-siRNA. Gef inhibited the EGFR signaling pathway, while YAP-siRNA suppressed the activation of the EGFR bypass signaling pathway, achieving effective tumor growth inhibition. Additionally, the strategy could be combined with photodynamic therapy, inducing apoptosis by downregulating hypoxia-inducible factor-1 alpha (HIF-1α) [104]. Gou et al. used silk fibroin (SF) and gelatin as raw materials, employing gelatin to induce liquid-liquid phase separation of SF, and developed suitable GSC nanoparticles (Fig. 6) [105]. These nanoparticles possess broad-spectrum drug delivery capabilities and, when administered through aerosolization, exhibit matrix metalloproteinase-9 (MMP-9) responsiveness in cells. They also demonstrate certain immunomodulatory properties, such as promoting the polarization of macrophages to the M1 phenotype and the maturation of dendritic cells, thereby enhancing immune responses and showing significant therapeutic effects [101].

IPF is a chronic and progressive lung disease characterized by the formation of scars and fibrous tissue in the lung tissue, resulting in gradual deterioration of lung function [106]. IPF typically renders the lungs stiff, fragile, and impairs effective gas exchange [107]. Although the etiology of IPF remains incompletely understood, it is often associated with environmental and genetic factors. Individuals who have been exposed to harmful gases or particulate matter (such as asbestos, silica dust, and pollutants) over extended periods, smoking, infections, or autoimmune diseases are highly susceptible to developing this condition [108]. Currently, the treatment for IPF remains challenging as there are no specific medications available to completely reverse the progression of this disease.
In clinical practice, the primary goal of IPF treatment is generally to slow disease progression, alleviate symptoms, and improve patients' quality of life. Treatment modalities mainly include the use of immunosuppressants, corticosteroids, and anti-fibrotic drugs, oxygen therapy, as well as lung transplantation. Additionally, adjunctive therapies such as exercise rehabilitation and supportive care can also help patients manage the disease and improve their quality of life [109]. Immunomodulators such as cyclosporine can control overactive immune responses and reduce inflammation. The anti-fibrotic drugs like nintedanib and pirfenidone have been approved by U.S. Food and Drug Administration (FDA) for treating specific types of pulmonary fibrosis [110]. Oxygen therapy involves providing sufficient oxygen to alleviate shortness of breath and symptoms of hypoxia [111].
However, these traditional treatment approaches cannot fully repair the damaged lung tissue. Some small molecule drugs, such as inhaled corticosteroids, anti-fibrotic drugs or immunosuppressants, often come with side effects including immune suppression, osteoporosis, and susceptibility to infections [112]. Moreover, patients with IPF may develop resistance to therapeutic agents, leading to decreased their efficacy.
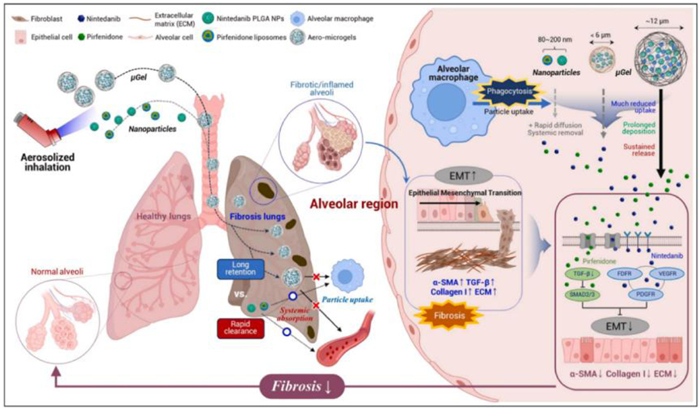
Patel et al. developed lipid-polymer hybrid nanoparticles (LPHNPs) loaded with nintedanib esylate (NE) using a nanoprecipitation method and optimized them through Box-Behnken design (BBD) [113]. These nanoparticles are administered in powder form for inhalation therapy. Through tissue uptake studies, it was found that LPHNPs exhibit high deposition in the alveolar regions, indicating that NE-loaded LPHNPs can effectively enhance local drug delivery. Local delivery allows the drug to be applied directly to the target area, resulting in significantly higher drug concentrations in that region compared to systemic delivery. This reduces systemic drug absorption, thereby decreasing the risk of systemic side effects, while achieving higher drug concentrations in the affected area, which may lead to better efficacy. In addition to using the nanoprecipitation method to prepare NE-loaded LPHNPs, Park et al. used PLGA-based discoidal polymeric particles (Nib-PLGA-DPPs) for NE delivery in IPF treatment [114]. Discoidal polymeric particles loaded with PLGA were synthesized using a top-down approach. PLGA and NE were dissolved in respective solvents, then uniformly mixed and cast into a PVA template with disk-shaped wells. After drying, dissolution, and filtration, Nib-PLGA-DPPs were obtained. These nanoparticles allow for modulation of NE release rate by adjusting the lactide molar ratio; a higher ratio results in slower release, higher drug utilization, and reduced lung inflammation and fibrosis. Biomedical polymers can not only deliver antibiotic drugs for treating pulmonary fibrosis but can also deliver gene therapies such as siRNA with promising results [115]. Adams et al. designed and synthesized poly(spermine acrylamides) (P(SpAA)) through polymerization with N-acryloxysuccinimide (NAS) and N-decylacrylamide (DAA), and then converted the active ester to a spermine-based pendant group [116]. Co-polymerization with dodecyl acrylamide increased the polymer's hydrophobicity. After deprotection, siRNA was encapsulated in the polymer. The siRNA delivery performance was demonstrated to be superior in vitro and in human lung xenografts, achieving more effective silencing of proteinase-activated receptor 2 (PAR2) gene, providing an effective approach for the treatment of pulmonary fibrosis. In the treatment of pulmonary fibrosis, nebulized drug delivery is also an extremely important method. Lee et al. developed an inhalable nanogel to improve the treatment of pulmonary fibrosis (Fig. 7) [117]. Hydrophobic and hydrophilic anti-fibrotic drugs, nintedanib and pirfenidone, were incorporated into PLGA nanoparticles and liposomes, respectively, to prepare inhalable nebulized microgels with a size of approximately 12 µm. These microgels have an extended retention time in the lungs, effectively slowing the progression of pulmonary fibrosis, inactivating fibroblasts, inhibiting transforming growth factor-beta (TGF-β) progression, and suppressing the production of extracellular matrix (ECM) components (collagen I and alpha-smooth muscle actin (α-SMA)), ultimately improving lung function. This approach could provide an effective strategy for treating pulmonary fibrosis and other respiratory diseases.
Asthma, commonly referred to as bronchial asthma, is a chronic respiratory system disease characterized by airway inflammation and narrowing, resulting in recurrent wheezing, shortness of breath, chest tightness, and coughing [118]. These symptoms typically occur in response to triggers such as allergens, respiratory infections, exercise, cold air, pollutants, or smoke exposure [119]. During asthma attacks, the muscles around the airways contract, i.e., bronchospasm, the airway lining becomes inflamed and excessive mucus is produced, leading to airflow obstruction and difficulty breathing [120]. The symptoms of patients with asthma can show from mild to severe and vary over time.
Medications for asthma include long-term control medications and rapid relief medications [121]. The former can be used to reduce inflammation and improve bronchiectasis, while the latter often helps relieve acute symptoms of asthma. Long-term control medications include inhaled corticosteroids, leukotriene modulators, and long-acting beta-2 agonists, which are used daily to reduce airway inflammation and prevent asthma symptoms. Rapid relief drugs include short-acting beta-2 agonists and anticholinergics, which are used during an asthma attack as needed to quickly relieve symptoms [122]. For severe or poorly controlled asthma, biologic therapy or oral corticosteroids may be required under the guidance of a specialist.
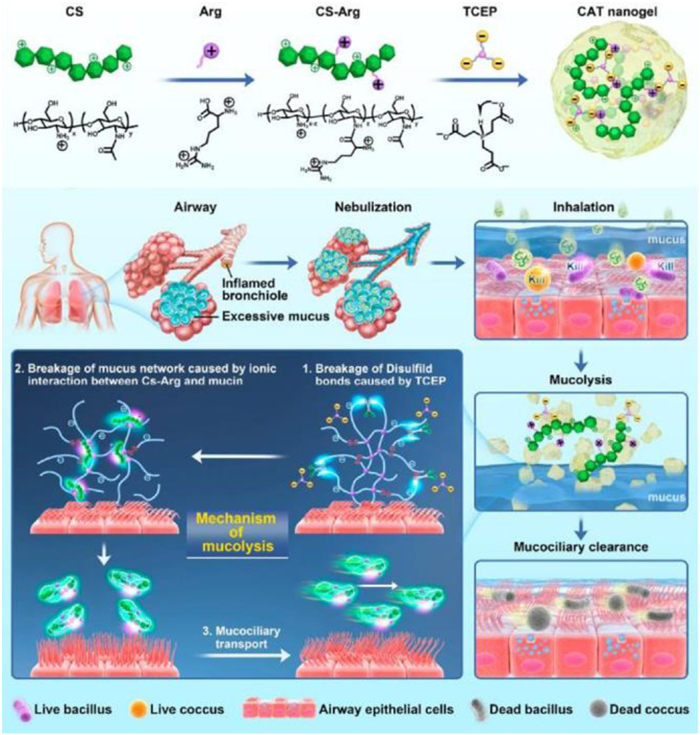
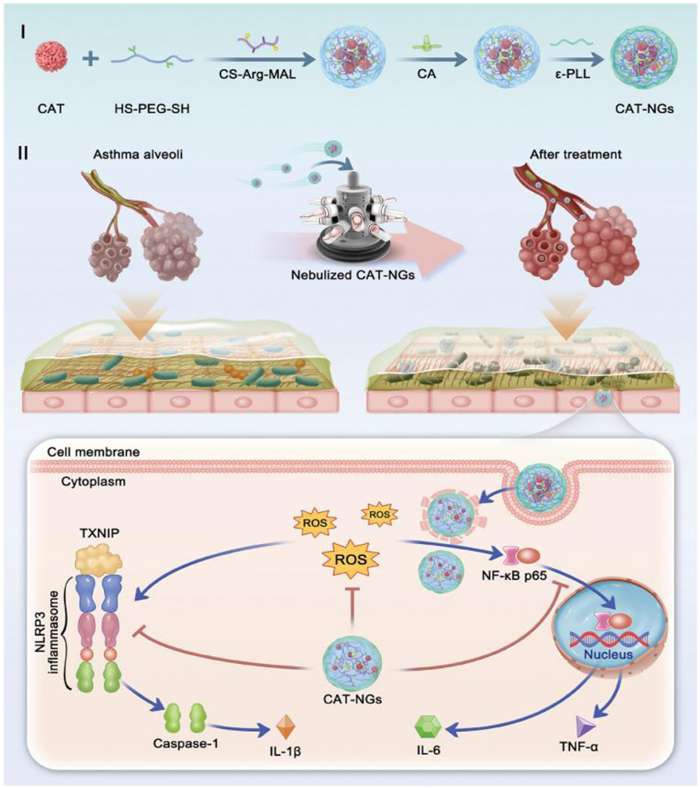
However, asthma is a stubborn disease often involving inflammation cell infiltration and mucus obstruction. Although small-molecule mucolytics have the ability to disrupt mucin protein disulfide bonds, their therapeutic efficacy in vivo is limited. Therefore, more effective treatment strategies are needed to prevent and manage asthma. Zhao et al. designed and prepared a mucolytic agent by developing a nano-gel composed of arginine-grafted chitosan (CS-Arg) cross-linked with tris(2-carboxyethyl)phosphine (TCEP). This nano-gel acts as a mucolytic agent, forming ionic interactions with mucins. It effectively inhibits the formation of large mucin aggregates in vitro, with the disulfide bonds in mucins being disrupted by the reducing TCEP (Fig. 8) [123]. In a mouse asthma model, the nano-gel administered via nebulization effectively alleviated mucus obstruction in the bronchioles and alveoli, reducing airway inflammation. Clinically, neutrophilic asthma is more severe than eosinophilic asthma and is often resistant to corticosteroids. Zuo et al. combined catalase with an antibacterial "protective film" to synthesize a novel nanogel (CAT-NGs) for catalase delivery. Compared to free catalase, CAT-NGs exhibit higher enzymatic activity and better resistance to trypsin. In a neutrophilic asthma mouse model, CAT-NGs, administered via aerosol treatment, significantly reduced lung inflammation and alleviated symptoms of neutrophilic asthma by scavenging reactive oxygen species (ROS) in the lungs and inhibiting the NOD-, LRR-, and pyrin domain-containing protein 3 (NLRP3) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) inflammatory pathways (Fig. 9) [124].
Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis that primarily affects lung tissue [125]. Spread by airborne droplets, Mycobacterium tuberculosis enters the human body through the respiratory tract [126], and close contact with patients is the most common route of infection. After diagnosis, tuberculosis patients should take anti-tuberculosis drugs for months or years to eradicate tuberculosis bacteria and prevent the disease from recurring [127]. The treatment of tuberculosis is often a long and complex process that requires close monitoring of treatment effects and adherence to prescribed treatment regimens. The drugs used to treat tuberculosis mainly include first-line drugs and adjuvant drugs. First-line drugs include isoniazid (INH), rifampicin (RIF), pyrazinamide (PZA), and ethambutol (EMB) [128,129]. Adjuvant drugs mainly include fluoroquinolones such as moxifloxacin, aminoglycosides such as amikacin (AM) and kanamycin, and ciprofloxacin. These drugs are often used in combination therapy to improve treatment effectiveness and reduce the development of drug resistance. Although anti-tuberculosis drugs can effectively inhibit and eliminate mycobacterium tuberculosis, they may also produce a series of side effects. Such as INH, RIF, PZA can cause abnormal liver function and gastrointestinal adverse reactions such as nausea and vomiting. EMB can lead to visual impairment, color vision abnormalities, eye movement disorders, and gastrointestinal discomfort [130,131]. To reduce the impact on other tissues and organs, we can design an appropriate microparticle to encapsulate the drug. This approach can increase accumulation at the lesion site and reduce side effects. Lokhande et al. prepared pH-responsive RIF microparticles containing lecithin and the biodegradable hydrophobic polymer polysebacic acid ester (PES) through a one-step precipitation method. These microparticles achieved an encapsulation efficiency of approximately 60%, demonstrated excellent macrophage uptake in RAW 264.7 macrophages, and exhibited enhanced anti-tuberculosis effects against intracellular Mycobacterium tuberculosis within macrophages. These microparticles hold promising potential for improving anti-tuberculosis efficacy [132]. Liao et al. processed RIF-loaded aggregation-induced emission (AIE) nanomicelles through sonication, filtration, and other treatments. In mouse or zebrafish tuberculosis models, these nanomicelles accumulated and released RIF within granulomas via the enhanced permeability and retention (EPR) effect. AIE molecules were used for targeted tracing and imaging, generating ROS upon light irradiation, which synergized with RIF to kill Mycobacterium tuberculosis (Fig. 10) [133]. This photodynamic synergistic chemotherapy method, which combines light-controlled ROS release and precise RIF delivery, effectively kills Mycobacterium tuberculosis and reduces drug side effects [133].

COPD is a general term for chronic lung diseases, including chronic bronchitis and emphysema. COPD is characterized by persistent airflow restriction and is a heterogeneous disease caused by the inhalation of cigarette smoke, toxic particles or gases [134]. At present, medication is the key to traditional COPD treatment. Commonly used drugs include bronchodilators and steroids. Bronchodilators can be used to dilate the airway and relieve respiratory symptoms [135]. Steroids administered by inhalation can effectively reduce pulmonary inflammation caused by COPD and reduce mucus production [136]. In addition, antibiotics are also used to treat respiratory infections caused by COPD [137] and mucus antidotes are used to relieve coughs. However, long-term use of steroids and long-acting bronchodilators often leads to serious side effects, such as decreased bone density and oral candidiasis [138]. While antibiotics are effective in treating respiratory infections caused by COPD, overuse of antibiotics can lead to antibiotic resistance problems. In addition, free small molecule drugs, when administered orally or intravenously, often lack tissue targeting in the lungs and may cause damage to normal tissues or organs [139].
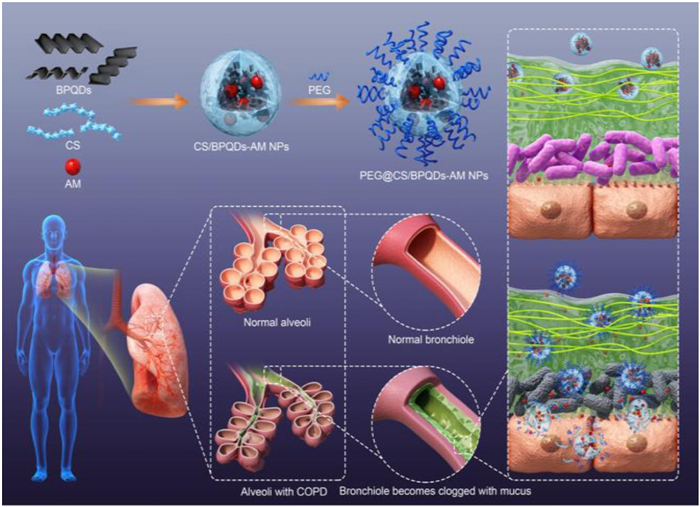
Therefore, we need to enhance the delivery efficiency of antibiotics as much as possible while minimizing damage to normal tissues or organs. To ensure that the nanocarrier can penetrate the mucus layer smoothly, Li et al. combined black phosphorus quantum dots (BPQDs) with AM-loaded polyhydroxy chitosan nanospheres (termed PEG@CS/BPQDs-AM NPs) [140]. Due to the hydrophilicity of PEG and the positive charge of CS, the nanocarrier penetrates the mucus layer and subsequently adheres to the mucosa. Meanwhile, BPQDs rapidly degrade into non-toxic PO43- and acidic H+, promoting the dissociation of the nanospheres and accelerating the release of AM, which then inactivates pathogenic bacteria (Fig. 11) [140]. This study demonstrates that BPQD-mediated drug delivery is a viable precision medicine strategy that not only enhances the release of the antibiotic AM but also reduces damage to other tissues and organs. Zhu et al. developed a dual-permeable immuno-antibacterial agent for mucus and bacterial biofilms (IMAMs), which possesses conditional bactericidal activity and extracellular DNA (eDNA)/genomic DNA (gDNA) inhibitory capabilities and can be used for aerosol treatment of COPD (Fig. 12) [141]. IMAMs consist of hollow mesoporous silica nanoparticles (HMSN) encapsulating ceftazidime (CAZ) and are functionalized with polypeptides bearing positively charged quaternary ammonium and negatively charged carboxyl groups in their side chains. The presence of amide bonds imparts pH-sensitive properties to the material, enabling flexible charge inversion and state change in different environments, which facilitates the proper release of the drug. At neutral pH, the electrostatic attraction between the side chains results in a negative charge and a random coil conformation of the polypeptides, which stack on the HMSN surface and prevent CAZ leakage. In an acidic environment, such as in COPD-afflicted mice, the negatively charged IMAMs effectively penetrate mucus and biofilms due to electrostatic repulsion with glycoproteins and polysaccharides. As the carboxyl groups on the negatively charged polypeptides are removed, the flexible random coils transition into positively charged, rigid α-helices capable of disrupting bacterial membranes, and CAZ is released from the silica mesopores. The combined action of the rigid α-helix and CAZ not only eradicates goblet bacteria but also effectively inhibits bacterial eDNA and gDNA, which suppresses immune cell infiltration and activation, avoid excessive activation of Toll-like receptor 9 (TLR9) in various types of immune cells, thereby promoting the resolution of inflammation caused by COPD.

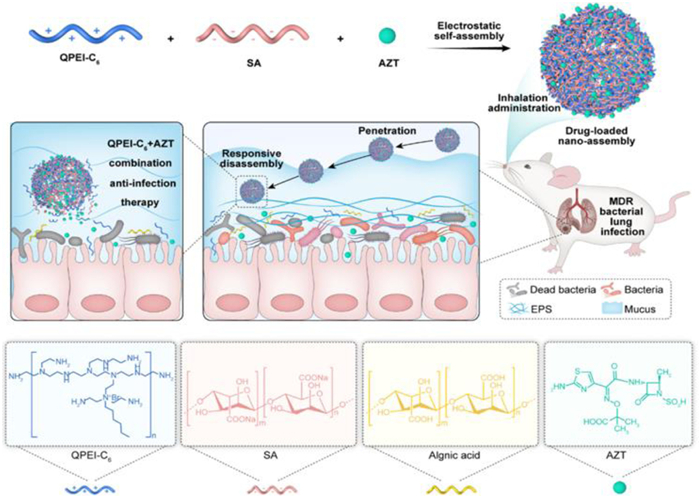
Due to the unique physiological structure of the lungs, air enters the lungs through the nasal or oral cavity [142]. When an infected person coughs or sneezes, pathogens can be transmitted through droplets into the air, potentially causing the spread of lung diseases. During lung infections, the immune system may fail to promptly recognize and attack the pathogens, increasing the risk of infectious diseases. In response to such infectious diseases, timely measures must be taken, such as isolating infected individuals from non-infected ones to reduce the risk of pathogen transmission. It is also crucial to avoid gathering in crowded and poorly ventilated environments, where pathogens spread more rapidly and infect a broader range of people. COVID-19, as a significant global public health event in recent years, has had widespread and highly destructive impacts worldwide [143]. The application of biomedical polymer materials to combat such diseases has played a critical role in mitigating the effects of COVID-19. For example, the mRNA vaccine BNT162b2 developed by Pfizer/BioNTech uses lipid nanoparticles as carriers for mRNA, successfully delivering mRNA into human cells and contributing significantly to stabilizing the pandemic [144]. Lower respiratory tract infections caused by bacteria often require antibiotic treatment. However, traditional systemic administration of antibiotics suffers from low drug utilization rates and may cause damage to other parts of the body. Han et al. successfully designed an inhalable drug delivery nanosystem, STQ12, by leveraging the electrostatic interactions between the positively charged antimicrobial polymer quaternized polyethyleneimine (QPEI-C6) and the negatively charged sodium alginate and loading the antibiotic azithromycin (AZT) (Fig. 13) [145]. The nanosystem is capable of pH-responsive disassembly in the slightly acidic environment of the infection site, releasing AZT and QPEI-C6. This approach effectively reduces drug loss during delivery, achieving a synergistic effect in eradicating multidrug-resistant bacteria and treating lower respiratory tract infections.
Biomedical polymer materials still face many challenges if they want to be truly applied in clinical practice. Since the lungs are a dynamic biological environment, they are constantly affected by factors such as airflow, humidity, and temperature. The implant or delivery system needs to be able to maintain stability in this environment, preventing displacement or damage due to physiological changes or respiratory dynamics. It is also necessary to prevent possible mucus adhesion, blockage, or interference with drug release. For drug delivery systems, drug stability is an important consideration. In the lung environment, the drug can be affected by factors such as oxidation, humidity and temperature, and it is necessary to ensure that the drug can remain effective over a long period of time.
In the clinical application of biomedical polymer materials in the treatment of lung diseases, standardization is a key factor in ensuring safety, efficacy and reproducibility. The process of manufacturing biomedical polymer materials needs to follow a series of standards to ensure the quality and consistency of the product, including the production, processing, disinfection and other standards of the material. Standardized biocompatibility and toxicity assessment procedures are important to ensure that materials are safe for humans, including in vitro and in vivo assessments to assess the compatibility of materials in the lung environment. If it involves medical devices, such as artificial airways or stents, it is necessary to comply with the relevant medical device standards, which involves the design of the equipment, material selection, performance testing and so on. For biomedical polymer materials involved in drug delivery, relevant drug delivery system standards need to be followed, including drug packaging, release rate, stability and other standards. Clinical trials of biomedical polymer materials in the treatment of lung diseases need to comply with international and national clinical trial standards, which ensures the ethical, scientific and data reliability of the trials. Different countries and regions may have different regulatory requirements, including registration, approval, production quality control and other standards, biomedical polymer materials need to meet these requirements in order to be legally sold and used in the market. After a product is put on the market, monitoring and reporting systems need to be in place to track the performance, safety and effectiveness of the product, which helps to identify and address potential problems in a timely manner. Standardization helps to ensure that the application of biomedical polymer materials in the treatment of lung diseases is scientific and reliable, and facilitates the sharing of information and exchange of experience internationally. This can improve the overall level of the industry and ensure that patients benefit from the most advanced and safe treatments.
Traditional treatment, whether it is surgery or chemoradiotherapy combined with drug treatment, will cause huge damage to the body, which is difficult to heal after surgery, and the wound is easy to cause infection, the immunity is reduced, and the patient's mood is difficult to adjust, and the patient will face great pressure both physically and psychologically. Therefore, the role of biomedical polymer materials in the treatment of lung diseases is increasingly critical, through the screening of materials, reasonable design, in vivo and in vitro performance characterization, and then gradually transition to clinical application, the biomedical polymer materials designed in this process have the advantages of good biocompatibility, good targeting, and little damage. Biomedical polymer materials can be used to replace or repair damaged or missing tissues and organs, such as artificial joints, artificial heart valves and orthopedic implants. These materials help restore patients' physiological function and improve their quality of life. The design of biomedical polymer materials focuses on biocompatibility, that is, the interaction of the material with biological tissues. Good biocompatibility helps to reduce rejection and the immune response caused by the implant, thereby improving patient acceptance of the implant and reducing patient discomfort. Biomedical polymer materials can be used to prepare drug delivery systems that deliver drugs directly to the treatment site, improving treatment effectiveness and reducing the amount of drugs patients need to receive, thereby mitigating adverse reactions. Biomimetic design of biomedical polymer materials brings their physical and chemical properties closer to natural tissues, helping to improve the adaptability and stability of medical devices and implants. Through these applications, biomedical polymer materials not only improve the quality of life of patients, but also improve treatment outcomes, making an important contribution to progress and innovation in the medical field.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Dayang Xie: Writing – original draft. Qiannan Cao: Writing – original draft. Huapan Fang: Writing – review & editing, Funding acquisition. Yanhui Li: Writing – review & editing, Funding acquisition. Huayu Tian: Writing – review & editing, Funding acquisition.
The authors are thankful to the National Key Research and Development Program of China (No. 2021YFB3800900); Natural Science Foundation of Xiamen, China (No. 3502Z202371004); National Natural Science Foundation of China (Nos. 52473150, 51925305, 52173115, 51873208, 51833010, and 52203183); Fundamental Research Funds for the Central Universities (No. 20720230004); and the Talent Cultivation Project Funds for the Innovation Laboratory for Sciences and Technologies of Energy Materials of Fujian Province (No. HRTP-[2022]52).
H. Zhang, J. Liu, M. Li, et al., Chin. Chem. Lett. 35 (2024) 110020. doi: 10.1016/j.cclet.2024.110020
T. Karampitsakos, B.M. Juan-Guardela, A. Tzouvelekis, et al., eBioMedicine 95 (2023) 104766. doi: 10.1016/j.ebiom.2023.104766
P.J. Barnes, P.G.J. Burney, E.K. Silverman, et al., Nat. Rev. Dis. Primers 1 (2015) 15076. doi: 10.1038/nrdp.2015.76
F. Yan, X. Zhao, R. Li, et al., Chin. Chem. Lett. 35 (2024) 108504. doi: 10.1016/j.cclet.2023.108504
K.P. Hough, M.L. Curtiss, T.J. Blain, et al., Front. Med. 7 (2020) 191. doi: 10.3389/fmed.2020.00191
V.J. Munster, M. Flagg, M. Singh, et al., Sci. Adv. 7 (2021) eabj3627. doi: 10.1126/sciadv.abj3627
N.N. Alrajhi, Ann. Thorac. Med. 18 (2023) 173–181. doi: 10.4103/atm.atm_7_23
H. Shen, N. Zhang, Y.Q. Liu, et al., Front. Pharmacol. 12 (2022) 805535. doi: 10.3389/fphar.2021.805535
Q.N. Cao, H.P. Fang, H.Y. Tian, Biomaterials 310 (2024) 122628. doi: 10.1016/j.biomaterials.2024.122628
X.R. Fei, J.N. Liu, T. Liu, et al., Indian J. Pharm. Sci. 85 (2023) 90–101.
Y. Li, Y.L. Ma, Y.Y. Gao, D.D. Wang, Q. Chen, J. Thorac. Dis. 9 (2017) 1565–1573. doi: 10.21037/jtd.2017.05.42
Y.X. Pan, Y.X. Zhang, X.Y. Shi, et al., Sci. Bull. 68 (2023) 2779–2792. doi: 10.1016/j.scib.2023.10.004
M. Li, Y. Wang, L. Zhang, et al., ACS Nano 17 (2023) 16703–16714. doi: 10.1021/acsnano.3c03013
L. Yuan, L.D. Geng, D.F. Wu, et al., BMC Neurol. 22 (2022) 226. doi: 10.1186/s12883-022-02746-7
G. Li, M.H. Zhao, F. Xu, et al., Molecules 25 (2020) 5023. doi: 10.3390/molecules25215023
M.S. Singhvi, S.S. Zinjarde, D.V. Gokhale, J. Appl. Microbiol. 127 (2019) 1612–1626. doi: 10.1111/jam.14290
X.Y. Guo, Z.Y. Yang, H.P. Fang, et al., Chin. J. Polym. Sci. 42 (2024) 1699–1709. doi: 10.1007/s10118-024-3171-z
M.H. He, N. Nandu, T.B. Uyar, M. Royzen, M.V. Yigit, Chem. Commun. 56 (2020) 7313–7316. doi: 10.1039/D0CC03439H
C.S. Ulrik, S. Vijverberg, N.A. Hanania, Z. Diamant, Curr. Opin. Pulm. Med. 26 (2020) 33–39. doi: 10.1097/MCP.0000000000000639
P. Lilburn, J.P. Williamson, M. Phillips, et al., Intern. Med. J. 54 (2024) 204–213. doi: 10.1111/imj.16304
G. Bai, Y. Zhu, H. Cao, et al., Prog. Org. Coat. 197 (2024) 108748. doi: 10.1016/j.porgcoat.2024.108748
A. Volpe, U. Krishnan, M.S. Chiriacò, et al., Engineering 7 (2021) 1434–1440. doi: 10.1016/j.eng.2020.10.012
J.C. Schittny, Cell Tissue Res. 367 (2017) 427–444. doi: 10.1007/s00441-016-2545-0
C.C.W. Hsia, D.M. Hyde, E.R. Weibel, Compr. Physiol. 6 (2016) 827–895. doi: 10.1002/j.2040-4603.2016.tb00698.x
S. Singh, M. Bodas, N.K. Bhatraju, et al., Am. J. Physiol. Lung Cell Mol. Physiol. 310 (2016) L837–L845. doi: 10.1152/ajplung.00091.2015
M. Beaume, V. Lazarevic, T. Köhler, et al., Front. Microbiol. 7 (2016) 1749.
D. Antin-Ozerkis, A. Rubinowitz, J. Evans, R.J. Homer, R.A. Matthay, Clin. Chest. Med. 33 (2012) 123–149. doi: 10.1016/j.ccm.2012.01.004
M. Ochs, L.R. Nyengaard, A. Lung, et al., Am. J. Respir. Crit. Care Med. 169 (2004) 120–124. doi: 10.1164/rccm.200308-1107OC
Y. Kobayashi, T. Uehara, K. Kawasaki, et al., Clin. Anat. 28 (2015) 227–234. doi: 10.1002/ca.22463
P. Zarogoulidis, K. Darwiche, L. Yarmus, et al., Med. Chem. 10 (2014) 123–136. doi: 10.2174/157340641130900041
P.C. Calder, R. Albers, J.M. Antoine, et al., Br. J. Nutr. 101 (2009) S1–S45. doi: 10.1017/S0007114509990511
E.Y. Gusev, N.V. Zotova, Curr. Pharm. Des. 25 (2019) 251–297. doi: 10.2174/1381612825666190319114641
L. Chan, N. Karimi, S. Morovati, et al., Viruses 13 (2021) 2318. doi: 10.3390/v13112318
J.H. Comroe, Sci. Am. 214 (1966) 56–71. doi: 10.1038/scientificamerican0266-56
H.H. Popper, Cancer Metastasis Rev. 35 (2016) 75–91. doi: 10.1007/s10555-016-9618-0
E. Hulsey, T. Bland, Vaccine 33 (2015) 2546–2550. doi: 10.1016/j.vaccine.2015.04.020
S. Zimm, G.L. Wampler, D. Stablein, T. Hazra, H.F. Young, Cancer 48 (1981) 384–394. doi: 10.1002/1097-0142(19810715)48:2<384::AID-CNCR2820480227>3.0.CO;2-8
T.V. Petrova, G.Y. Koh, Science 369 (2020) eaax4063.
Z. Liang, R. Ni, J. Zhou, S. Mao, Drug Discov. Today 20 (2015) 380–389. doi: 10.1016/j.drudis.2014.09.020
X. Murgia, C. de Souza Carvalho, C.M. Lehr, Eur. J. Nanomed. 6 (2014) 157–169. doi: 10.1515/ejnm-2014-0019
J.H. Widdicombe, J.J. Wine, Physiol. Rev. 95 (2015) 1241–1319. doi: 10.1152/physrev.00039.2014
W. Zhang, J. Hughes, Y. Chen, Appl. Environ. Microbiol. 78 (2012) 3905–3915. doi: 10.1128/AEM.00193-12
K. Roe, Clin. Chim. Acta 563 (2024) 119889. doi: 10.1016/j.cca.2024.119889
J. Jagur-Grodzinski, Polym. Adv. Technol. 17 (2006) 395–418. doi: 10.1002/pat.729
Y.Q. Zhu, C. Romain, C.K. Williams, Nature 540 (2016) 354–362. doi: 10.1038/nature21001
A. Sionkowska, K. Adamiak, K. Musial, M. Gadomska, Materials 13 (2020) 4217. doi: 10.3390/ma13194217
B. Jadach, Z. Mielcarek, T. Osmalek, Curr. Issues Mol. Biol. 46 (2024) 2043–2070. doi: 10.3390/cimb46030132
C.J. Dong, Y.G. Lv, Polymers 8 (2016) 42. doi: 10.3390/polym8020042
M. Aprilliza Helmiyati, Int. Symp. Curr. Prog. Funct. Mater. 188 (2016) 012019.
H.Y. Li, Alginate-based inhalable particles for controlled pulmonary drug delivery, in: S. Jana, S. Jana (Eds.), Alginate Biomaterial: Drug Delivery Strategies and Biomedical Engineering, Springer Nature Singapore, Singapore, 2023, pp. 207–240.
M. Alnaief, R.M. Obaidat, M.M. Alsmadi, Polymers 12 (2020) 2223. doi: 10.3390/polym12102223
S. Bensouiki, F. Belaib, M. Sindt, et al., Arabian J. Sci. Eng. 45 (2020) 7599–7609. doi: 10.1007/s13369-020-04720-2
H. Fang, L. Chen, Z. Deng, et al., ACS Nano 17 (2023) 1128–1143. doi: 10.1021/acsnano.2c08434
B. Tyler, D. Gullotti, A. Mangraviti, T. Utsuki, H. Brem, Adv. Drug Deliv. Rev. 107 (2016) 163–175. doi: 10.1016/j.addr.2016.06.018
M. Smola, T. Vandamme, A. Sokolowski, Int. J. Nanomed. 3 (2008) 1–19.
F. Emami, S.J. Mostafavi Yazdi, D.H. Na, J. Pharm. Invest. 49 (2019) 427–442. doi: 10.1007/s40005-019-00443-1
K.A. Athanasiou, G.G. Niederauer, C.M. Agrawal, Biomaterials 17 (1996) 93–102. doi: 10.1016/0142-9612(96)85754-1
M.S. Zafar, Polymers 12 (2020) 2299. doi: 10.3390/polym12102299
A. Bettencourt, A.J. Almeida, J. Microencapsulation 29 (2012) 353–367. doi: 10.3109/02652048.2011.651500
H.P. Fang, Z.P. Guo, L. Lin, et al., J. Am. Chem. Soc. 140 (2018) 11992–12000. doi: 10.1021/jacs.8b05341
J.P. Eubeler, S. Zok, M. Bernhard, T.P. Knepper, TrAC Trends Anal. Chem. 28 (2009) 1057–1072. doi: 10.1016/j.trac.2009.06.007
E. Fournier, C. Passirani, C.N. Montero-Menei, J.P. Benoit, Biomaterials 24 (2003) 3311–3331. doi: 10.1016/S0142-9612(03)00161-3
A. Balde, S.K. Kim, S. Benjakul, R.A. Nazeer, Int. J. Biol. Macromol. 220 (2022) 1464–1479. doi: 10.1016/j.ijbiomac.2022.09.116
M. Harun-Or-Rashid, M.N. Aktar, M.S. Hossain, Polymers 15 (2023) 4563. doi: 10.3390/polym15234563
W. Friess, Eur. J. Pharm. Biopharm. 45 (1998) 113–136. doi: 10.1016/S0939-6411(98)00017-4
A. Santos, F. Veiga, A. Figueiras, Materials 13 (2020) 65.
H.W. Toh, D.W.Y. Toong, J.C.K. Ng, et al., Eur. Polym. J. 146 (2021) 110249. doi: 10.1016/j.eurpolymj.2020.110249
J. Li, D.J. Mooney, Nat. Rev. Mater. 1 (2016) 16071. doi: 10.1038/natrevmats.2016.71
M.L.W. Knetsch, L.H. Koole, Polymers 3 (2011) 340–366. doi: 10.3390/polym3010340
F. Furno, K.S. Morley, B. Wong, et al., J. Antimicrob. Chemother. 54 (2004) 1019–1024. doi: 10.1093/jac/dkh478
S. Zhang, H. Fang, H. Tian, Biomacromolecules 25 (2024) 7015–7057. doi: 10.1021/acs.biomac.4c01193
C. Li, S. Lei, L. Ding, Chin. Med. J. 136 (2023) 1583–1590. doi: 10.1097/CM9.0000000000002529
H. Liang, X. Zhou, Y. Zhu, Environ. Res. 218 (2023) 114996. doi: 10.1016/j.envres.2022.114996
G.S.B. Aseervatham, T. Sivasudha, R. Jeyadevi, D. Arul Ananth, Environ. Sci. Pollut. Res. 20 (2013) 4356–4369. doi: 10.1007/s11356-013-1748-0
C. Zappa, S.A. Mousa, Transl. Lung Cancer Res. 5 (2016) 288–300. doi: 10.21037/tlcr.2016.06.07
P.A. Kvale, P.A. Selecky, U.B.S. Prakash, Chest 132 (2007) 368S–403S. doi: 10.1378/chest.07-1391
F.R. Hirsch, G.V. Scagliotti, J.L. Mulshine, et al., Lancet 389 (2017) 299–311. doi: 10.1016/S0140-6736(16)30958-8
C.F.J. Yang, T.A. D'Amico, Ann. Thorac. Surg. 94 (2012) 668–681. doi: 10.1016/j.athoracsur.2012.03.080
J.E. Coggle, B.E. Lambert, S.R. Moores, Environ. Health Perspect. 70 (1986) 261–291. doi: 10.1289/ehp.8670261
L. Jiao, C. Dong, J. Liu, et al., Sci. Rep. 7 (2017) 46524. doi: 10.1038/srep46524
Y.T. Lee, Y.J. Tan, C.E. Oon, Eur. J. Pharmacol. 834 (2018) 188–196. doi: 10.1016/j.ejphar.2018.07.034
H. Abdel-Razeq, H. Hashem, Crit. Rev. Oncol. Hematol. 145 (2020) 102837. doi: 10.1016/j.critrevonc.2019.102837
M. Aldea, F. Andre, A. Marabelle, et al., Cancer Discov. 11 (2021) 874–899. doi: 10.1158/2159-8290.CD-20-1638
S. Boumahdi, F.J. de Sauvage, Nat. Rev. Drug Discov. 19 (2020) 39–56. doi: 10.1038/s41573-019-0044-1
M. Riihimäki, A. Hemminki, M. Fallah, Lung Cancer 86 (2014) 78–84. doi: 10.1016/j.lungcan.2014.07.020
R. Salgia, T. Hensing, N. Campbell, Semin. Oncol. 38 (2011) 274–283. doi: 10.1053/j.seminoncol.2011.01.012
H.P. Fang, Q. Chen, Matter 5 (2022) 2423–2425. doi: 10.1016/j.matt.2022.05.016
S. Doppalapudi, A. Jain, A.J. Domb, W. Khan, Expert Opin. Drug Deliv. 13 (2016) 891–909. doi: 10.1517/17425247.2016.1156671
M. Elsabahy, K.L. Wooley, Chem. Soc. Rev. 41 (2012) 2545–2561. doi: 10.1039/c2cs15327k
H.P. Fang, Z.P. Guo, J. Chen, Nat. Commun. 12 (2021) 6742. doi: 10.1038/s41467-021-27078-x
A. Jain, S.K. Singh, S.K. Arya, S.C. Kundu, S. Kapoor, ACS Biomater. Sci. Eng. 4 (2018) 3939–3961. doi: 10.1021/acsbiomaterials.8b01098
B. Yadav, M. Chauhan, S. Shekhar, et al., Int. J. Pharm. 633 (2023) 122587. doi: 10.1016/j.ijpharm.2023.122587
F. Danhier, E. Ansorena, J.M. Silva, et al., J. Control. Release 161 (2012) 505–522. doi: 10.1016/j.jconrel.2012.01.043
J.B. Opalinska, A.M. Gewirtz, Nat. Rev. Drug Discov. 1 (2002) 503–514. doi: 10.1038/nrd837
H.P. Fang, J. Chen, L. Lin, ACS Appl. Mater. Interfaces 11 (2019) 47785–47797. doi: 10.1021/acsami.9b18144
H.P. Fang, H.Y. Tian, X.S. Chen, J. Control. Release 259 (2017) E47.
L. Xu, T. Anchordoquy, J. Pharm. Sci. 100 (2011) 38–52. doi: 10.1002/jps.22243
H. Fang, L. Lin, J. Chen, et al., Biomater. Sci. 7 (2019) 1716–1728. doi: 10.1039/C9BM00039A
Z. Ma, S. Wong, H. Forgham, Biomaterials 285 (2022) 121539. doi: 10.1016/j.biomaterials.2022.121539
J. Teo, J.A. McCarroll, C. Boyer, Biomacromolecules 17 (2016) 2337–2351. doi: 10.1021/acs.biomac.6b00185
Y. Qin, L. Ou, L. Zha, Y. Zeng, L. Li, Mol. Biomed. 4 (2023) 48. doi: 10.1186/s43556-023-00160-0
N.D. Le, B.L. Nguyen, B.R. Patil, et al., ACS Nano 18 (2024) 8392–8410. doi: 10.1021/acsnano.3c13039
L. Rotolo, D. Vanover, N.C. Bruno, et al., Nat. Mater. 22 (2023) 369–379. doi: 10.1038/s41563-022-01404-0
J.X. Huang, C. Zhuang, J. Chen, et al., Adv. Mater. 34 (2022) e2201516. doi: 10.1002/adma.202201516
S.Q. Gou, G.Y. Wang, Y.A. Zou, et al., Adv. Mater. 35 (2023) e2303718. doi: 10.1002/adma.202303718
F.J. Martinez, H.R. Collard, A. Pardo, et al., Nat. Rev. Disease Primers 3 (2017) 17074. doi: 10.1038/nrdp.2017.74
N. Berend, Respirology 19 (2014) 952–959. doi: 10.1111/resp.12348
A. Duck, L.G. Spencer, S. Bailey, J. Adv. Nurs. 71 (2015) 1055–1065. doi: 10.1111/jan.12587
R.H. Zou, D.J. Kass, K.F. Gibson, K.O. Lindell, Pulm. Ther. 6 (2020) 35–46. doi: 10.1007/s41030-019-00108-2
A. Gunatilaka, S. Zhang, W.S.D. Tan, A.G. Stewart, Adv. Pharmacol. 98 (2023) 179–224.
Y. Lacasse, A.Y.M. Tan, F. Maltais, J.A. Krishnan, Am. J. Respir. Crit. Care Med. 197 (2018) 1254–1264. doi: 10.1164/rccm.201802-0382CI
A.S. Melani, C. Bigliazzi, F.A. Cimmino, L. Bergantini, E. Bargagli, Pulm. Ther. 7 (2021) 325–344. doi: 10.1007/s41030-021-00160-x
M. Patel, S. Karampuri, V. Kansara, B. Vyas, J. Drug Deliv. Sci. Technol. 86 (2023) 104716. doi: 10.1016/j.jddst.2023.104716
S. Park, J.Y. Park, J.H. Nahm, et al., Mater. Today Chem. 26 (2022) 101181. doi: 10.1016/j.mtchem.2022.101181
H. Fang, Y. Wu, L. Chen, et al., ACS Nano 17 (2023) 4748–4763. doi: 10.1021/acsnano.2c11159
F. Adams, C.M. Zimmermann, D. Baldassi, et al., Small 20 (2024) 2308775. doi: 10.1002/smll.202308775
W.T. Lee, H.Y.J. Lee, J. Kim, et al., Bioact. Mater. 33 (2024) 262–278.
J.H. Krouse, R.W. Brown, S.M. Fineman, et al., Otolaryngol. Head Neck Surg. 136 (2007) S75–S106.
M.K. Vernon, I. Wiklund, J.A. Bell, P. Dale, K.R. Chapman, J. Asthma 49 (2012) 991–998. doi: 10.3109/02770903.2012.738268
G.G. King, P.D. Paré, C.Y. Seow, Respir. Physiol. 118 (1999) 1–13.
N. Walders, S.J. Kopel, D. Koinis-Mitchell, E.L. McQuaid, J. Pediatr. 146 (2005) 177–182. doi: 10.1016/j.jpeds.2004.10.014
B.F. Chauhan, F.M. Ducharme, Cochrane Database Syst. Rev. 2014 (2014) CD003137.
D. Zhao, D. Li, X.L. Cheng, ACS Nano 16 (2022) 11161–11173. doi: 10.1021/acsnano.2c03993
X. Zuo, X.P. Guo, Y.N. Gu, Adv. Funct. Mater. 34 (2024) 2316496. doi: 10.1002/adfm.202316496
G. Delogu, M. Sali, G. Fadda, Mediterr. J. Hematol. Infect. Dis. 5 (2013) e2013070. doi: 10.4084/mjhid.2013.070
M.U. Shiloh, Future Microbiol. 11 (2016) 1503–1506. doi: 10.2217/fmb-2016-0185
S. Liu, W. Wei, Prevention, diagnosis, and treatment of TB in the migrating population, in: W. Yu, P. Lu, W. Tan (Eds.), Tuberculosis Control in Migrating Population, Springer Singapore, Singapore, 2020, pp. 63–96.
A. Zumla, J. Chakaya, R. Centis, et al., Lancet Respir. Med. 3 (2015) 220–234. doi: 10.1016/S2213-2600(15)00063-6
A. Amin, A. Vartanian, A. Yegiazaryan, A.L. Al-Kassir, V. Venketaraman, Infect. Dis. Rep. 13 (2021) 821–834. doi: 10.3390/idr13030074
Y. Xu, J. Wu, S. Liao, Z. Sun, Ann. Clin. Microbiol. Antimicrob. 16 (2017) 67. doi: 10.1186/s12941-017-0239-4
G. Ramachandran, S. Swaminathan, Drug Saf. 38 (2015) 253–269. doi: 10.1007/s40264-015-0267-y
A.S. Lokhande, F. Panchal, R. Munshi, Int. J. Pharm. 635 (2023) 122729. doi: 10.1016/j.ijpharm.2023.122729
Y.H. Liao, B. Li, Z. Zhao, ACS Nano 14 (2020) 8046–8058. doi: 10.1021/acsnano.0c00586
I.A. Yang, C.R. Jenkins, S.S. Salvi, Lancet Respir. Med. 10 (2022) 497–511. doi: 10.1016/S2213-2600(21)00506-3
M. Cazzola, C.P. Page, L. Calzetta, M.G. Matera, Pharmacol. Rev. 64 (2012) 450–504. doi: 10.1124/pr.111.004580
H.R. Keir, M. Contoli, J.D. Chalmers, Biomedicines 9 (2021) 1312. doi: 10.3390/biomedicines9101312
M. Miravitlles, A. Anzueto, Int. J. Mol. Sci. 18 (2017) 1344. doi: 10.3390/ijms18071344
M. Miravitlles, A. Auladell-Rispau, M. Monteagudo, et al., Eur. Respir. Rev. 30 (2021) 210075. doi: 10.1183/16000617.0075-2021
M.X. Gu, S.D. Sun, Q.D. You, L. Wang, Molecules 28 (2023) 7941. doi: 10.3390/molecules28247941
Z.B. Li, G.H. Luo, W.P. Hu, et al., Angew. Chem. Int. Ed. 59 (2020) 20568–20576. doi: 10.1002/anie.202008379
J.L. Zhu, X.H. Li, Y. Zhou, et al., Sci. Adv. 10 (2024) eabd7904. doi: 10.1126/sciadv.abd7904
F. Lizal, J. Elcner, J. Jedelsky, et al., J. Aerosol Sci. 150 (2020) 105649. doi: 10.1016/j.jaerosci.2020.105649
Y. Miyah, M. Benjelloun, S. Lairini, A. Lahrichi, Sci. World J. 2022 (2022) 5578284.
C. Li, A. Lee, L. Grigoryan, et al., Nat. Immunol. 23 (2022) 543–555. doi: 10.1038/s41590-022-01163-9
L. Han, Z. Yuan, H.M. Ren, et al., BMEMat 2 (2024) e12082. doi: 10.1002/bmm2.12082

Figure 1 Number of publications on biomedical materials and pulmonary disease therapy in Web of Science from 2014 to Sep. 2024.

Figure 2 Applications of biomedical polymer materials in pulmonary diseases. Created with BioRender.

Figure 3 The synthesis of star nanoparticles, their distribution in tissues and organs after nebulization, and their therapeutic effects in vivo. (A) The synthetic route of star nanoparticles. (B) Fluorescent images of nebulized nanoparticles as siRNA carriers in various tissues and organs. (C) Hematoxylin and eosin (HE) images of nebulized nanoparticles carrying siPLK1 after treating in situ lung tumors. (D) Representative images of ex vivo lung bioluminescence and quantitative analysis. Reproduced with permission [99]. Copyright 2022, Elsevier.

Figure 4 Schematic representation of the proposed mechanism of PBAEs lipid nanoparticles containing mRNA encoding bevacizumab. After mixing the PBAEs lipid nanoparticles in the ethanol phase with mRNA in the acidic aqueous phase, the nanoparticles are administered intravenously into the mouse body. The nanoparticles target the lungs and enter the cells through cellular uptake, allowing the mRNA to exert its effects by encoding bevacizumab, which inhibits the production of VEGF. Reproduced with permission [102]. Copyright 2024, American Chemical Society.

Figure 5 The schematic diagram of anti-tumor effects of block and dendritic nanoparticles loaded with Gef and YAP-siRNA. In both CDX and PDX models, the nanoparticles can release Gef and YAP-siRNA in NSCLC cells, inhibiting the EGFR signaling pathway and EGFR bypass signaling pathway. Combined with photodynamic therapy, this can produce a potent anti-tumor effect. Copied with permission [104]. Copyright 2022, John Wiley and Sons.

Figure 6 A schematic diagram of the broad-spectrum drug-loading characteristics and tumor-specific therapy of GSC particles. Copied with permission [105]. Copyright 2023, John Wiley and Sons.

Figure 7 Schematic diagram of a nebulizable inhalable microgel containing nintedanib and pirfenidone. The microgel accumulates in the lungs, inhibits TGF-β, suppresses ECM, and improves lung function. Copied with permission [117]. Copyright 2024, Elsevier.

Figure 8 Diagram of preparation, atomization, and treatment of allergic asthma by adhesion and erosion of mucous networks and inactivation of bacteria of CAT nanogels. Reproduced with permission [123]. Copyright 2022, American Chemical Society.

Figure 9 Schematic diagram of the preparation and mechanism of action of CAT-NGs nanogel, which alleviates neutrophilic asthma by scavenging ROS in the lungs and inhibiting the NLRP3 and NF-κB inflammatory pathways. Copied with permission [124]. Copyright 2024, John Wiley and Sons.

Figure 10 Schematic diagram of the function of RIF-loaded AIE nanomicelles. Copied with permission [133]. Copyright 2020, American Chemical Society.

Figure 11 A schematic of the preparation of PEG@CS/BPQDs-AM NPs shows that the nanocarrier smoothly penetrates the mucus layer, and with the dissociation of the nanospheres, AM is rapidly released to kill pathogenic bacteria. Copied with permission [140]. Copyright 2020, John Wiley and Sons.

Figure 12 Schematic of IMAMs preparation. (A) In different pH environments, polypeptides with negatively charged carboxyl groups exhibit distinct conformations. (B) Diagram of IMAMs action. In COPD mice, the random coil polypeptide transitions into a rigid α-helix due to carboxyl group removal, releasing CAZ. This combined treatment kills pathogenic bacteria, inhibits bacterial eDNA and gDNA, and promotes the resolution of COPD-induced inflammation. Copied with permission [141]. Copyright 2024, The American Association for the Advancement of Science.

Figure 13 The synthetic route and mechanism diagram of STQ12. STQ12 can disassemble in a mildly acidic environment, releasing AZT and QPEI-C6. The two compounds work synergistically to kill drug-resistant bacteria and treat lower respiratory tract infections. Copied with permission [145]. Copyright 2024, John Wiley and Sons.

 扫一扫看文章
扫一扫看文章

扫一扫关注我们
 DownLoad:
DownLoad:
 下载:
下载: