Citation:
Chunlei Hui, Xiuqing Li, Ying Liang, Qingqiu Huang, Li Fan, Li Su, Yuanqing Gao. Nasal gel-delivered adenosine A1 receptor agonist induces torpor-like hypothermia and improves survival in a hemorrhagic shock model[J]. Chinese Chemical Letters,
2026, 37(2): 111017.
doi:
10.1016/j.cclet.2025.111017
Nasal gel-delivered adenosine A1 receptor agonist induces torpor-like hypothermia and improves survival in a hemorrhagic shock model
English
Nasal gel-delivered adenosine A1 receptor agonist induces torpor-like hypothermia and improves survival in a hemorrhagic shock model
Received Date:
02 December 2024 Accepted Date:
27 February 2025 Revised Date:
24 February 2025 Available Online:
15 February 2026
Abstract:
Hemorrhagic shock (HS) is a leading cause of death worldwide, particularly within the first 24 h post-injury. Current treatments are limited, especially in low-resource settings. Therapeutic hypothermia (TH) offers potential benefits by reducing metabolic demands and protecting organs, but its application in HS is challenged by cooling difficulties and side effects. This study introduces a novel nasal gel formulation of N6-cyclohexyladenosine (CHA), an adenosine A1 receptor agonist, designed to enhance brain delivery while minimizing peripheral side effects. In a mouse model of HS, administration of CHA nasal gel significantly improved survival rates, reduced metabolic rates, and protected major organs without worsening coagulopathy. Metabolomics analysis revealed a shift towards fatty acid oxidation and increased antioxidant capacity. These findings demonstrate that CHA nasal gel effectively induces TH, offering a safe and innovative treatment strategy for HS, particularly in resource-limited environments.
Hemorrhagic shock (HS) is a major cause of mortality worldwide, significantly contributing to deaths both on the battlefield and among civilian populations [1,2]. Hemorrhage is responsible for 30%–40% of deaths after trauma and 27% of maternal death [3]. Most hemorrhagic deaths occur within the first 24 h post-injury, predominantly within the initial 6 h [4]. Over the past few decades, the management of HS has evolved from basic fluid resuscitation to more advanced techniques such as damage control surgery and goal-directed therapy [5]. Despite technological advances, current treatments still fail to adequately address the needs of all patient demographics, particularly, in low-resource settings. This underscores the need for more adaptable and less resource-intensive solutions.
Therapeutic hypothermia (TH) has been investigated as a potential intervention for managing traumatic HS and ischemia-reperfusion injury by reducing metabolic demands and preserving major organ function [6]. TH is already used in certain clinical settings, such as cardiac arrest and neonatal encephalopathy traumatic brain injury, where it has demonstrated significant benefits [7,8]. However, its application in HS is challenged by difficulties in achieving rapid and controlled cooling, complex equipment requirements, and the risk of exacerbating coagulopathy and hemodynamic instability [9]. Thus, translating TH into clinical use for HS remains controversial, with innovative methods needed to overcome these obstacles.
While early studies explored moderate and deep hypothermia (<30 ℃), more recent research has shifted towards mild hypothermia (33–36 ℃) as a more feasible and safer strategy [10]. Torpor, characterized by a profound reduction in body temperature and metabolic rate, occurs naturally in some mammals [11]. Mimicking torpor in non-hibernating species has emerged as a potential therapeutic approach to induce a hypometabolism, offering protection against ischemic injury [12]. N6-cyclohexyladenosine (CHA), an adenosine A1 receptor agonist, has been shown to induce torpor-like hypothermia in rodents [13]. Our previous study demonstrates its therapeutic effect against neuroinflammation by preserving the integrity of blood-brain barrier upon infection [14]. Whether CHA could benefit HS remains unexplored. Additionally, systemic CHA administration may induce cardiovascular side effects due to peripheral A1 receptor activation, limiting its clinical utility.
Hydrogels have emerged as a promising approach for drug delivery due to their excellent biocompatibility, controlled release properties, and ability to facilitate targeted therapy [15-17]. Hydrogels have been successfully adapted for nasal drug delivery systems, where their ability to be rapidly absorbed and directly target brain tissues offers significant advantages in non-invasive therapeutic interventions. In this study, we first developed a CHA nasal gel for brain delivery, minimizing peripheral side effects and evaluated its efficacy and safety in inducing torpor-like hypothermia. Then, we assessed the therapeutic potential of CHA-induced hypothermia in a mouse model of HS. We observed that CHA significantly reduced mortality, lowered metabolic rates, and protected major organs without increasing coagulopathy risk. Metabolomics analysis revealed a shift towards fatty acid oxidation and enhanced antioxidant capacity. These findings demonstrate that CHA nasal gel is a viable method to induce TH, which offers a novel and effective treatment strategy for HS with minimal side effects.
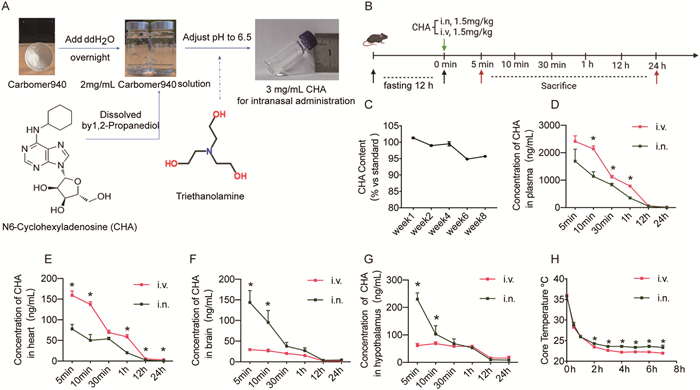
In our previous study, we demonstrated the efficacy of CHA in inducing torpor-like hypothermia. To minimize potential cardiovascular side effects, we developed a CHA nasal gel for targeted delivery to the brain. The preparation process is illustrated in Fig. 1A. We then compared the distribution of CHA in major organs following intranasal and intravenous administration (Fig. 1B) and quantified CHA using high-performance liquid chromatography (Fig. S1 in Supporting information). The CHA nasal gel maintained stability at room temperature, retaining over 95% of active CHA content after eight weeks of storage (Fig. 1C). Intranasal administration resulted in significantly lower CHA concentrations over time in plasma (Fig. 1D), and reduced accumulation in heart tissue compared to intravenous administration (Fig. 1E). Notably, intranasal administration led to significantly higher CHA concentrations in the brain compared to intravenous delivery (Fig. 1F), with a similar pattern observed in the hypothalamus which is responsible for temperature regulation (Fig. 1G). Both administration routes rapidly induced torpor-like hypothermia, with intravenous being slightly lower. However, considering the peripheral side effects associated with CHA, Intranasal administration is the preferred approach for minimizing adverse effects while achieving similar therapeutic outcomes (Fig. 1H). These results confirm that the CHA nasal gel is both effective and durable for therapeutic use.
Figure 1
Figure 1.
Preparation of a CHA nasal gel and its distribution dynamics. (A) The procedure of the preparation of CHA nasal gel. (B) Timeline of CHA administration intranasally (i.n.) or intravenously (i.v.) at a dose of 1.5 mg/kg. Blood and tissue samples were collected at various time points post-administration for analysis. (C) Stability test of CHA in the nasal gel formulation over 8 weeks. Concentration of CHA in plasma (D), heart (E), whole brain (F) and hypothalamus (G) over time following CHA administration. (H) Core temperature changes over time following CHA administration. Data are presented as mean ± SEM. Unpaired t-test was performed in all experiments. *P < 0.05.
To assess the safety of CHA nasal gel, as shown in Fig. S2 (Supporting information), we conducted histopathological and biochemical evaluations following a 7-day intranasal administration in guinea pigs (Fig. S2A). All the animal procedures were carried out in compliance with Shanghai University’s Guidelines for the Care and Use of Laboratory Animals (approved protocol No. ECSHU 2023–033). Histopathological analysis of the nasal mucosa, larynx, and trachea showed no significant structural damage between the CHA-treated group and the control group (Fig. S2B). Serum biochemical analysis indicated no statistically significant changes in liver and kidney function markers, including alanine transaminase (ALT), aspartate transaminase (AST), albumin (ALB), alkaline phosphatase (ALP), total protein (TP), blood urea nitrogen (BUN), creatinine (CREA), total bilirubin (TBIL) and creatine kinase (CK) (Figs. S2C–K). Lactate dehydrogenase (LDH) was elevated in the CHA group indicating a possible shift in energy metabolism shift (Fig. S2L). No pathological alterations were found in major organs, including the liver, kidney, spleen, heart, and lungs, further supporting the safety of CHA nasal gel at the tested dosage (Fig. S2M). In summary, we successfully formulated a stable CHA nasal gel that enhances brain delivery and achieves superior hypothermia induction compared to intravenous administration.
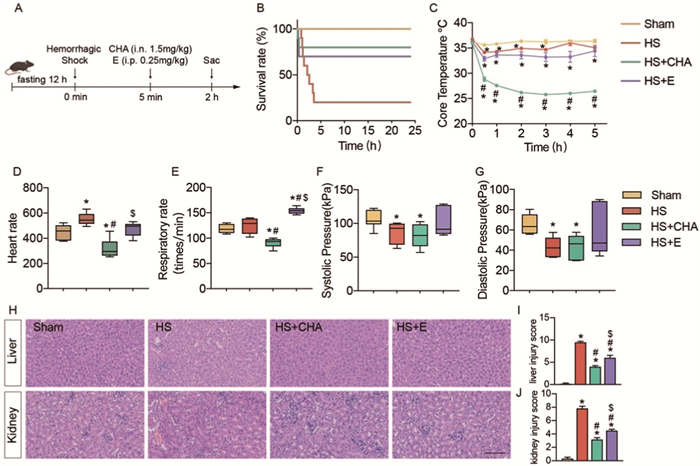
Next, we explored the therapeutic potential of CHA nasal gel in HS. We established a 40% fixed-volume hemorrhage model in C57 mice. CHA and epinephrine were administered 5 min post-hemorrhage (Fig. 2A). The survival rate was 20% in the HS group, while the CHA-treated group had an 80% survival rate, slightly higher than the epinephrine group (70%) (Fig. 2B). The core body temperature of CHA-treated mice rapidly dropped to approximately 25 ℃, maintaining a hypothermic state. The HS and epinephrine groups showed a slight decrease but remained around 34–35 ℃ (Fig. 2C). We measured heart rate, and respiratory rate and blood pressure after 2 h. CHA significantly reduced heart rate and respiratory rate compared to the HS group, whereas epinephrine increased respiratory rate. Both CHA and HS groups showed a drop in blood pressure, but CHA did not cause further decline (Figs. 2D–G), indicating that CHA does not exacerbate hypotension, a critical consideration in HS management. Histological analysis of liver and kidney tissue (Fig. 2H) revealed extensive damage in the HS group, including cellular degeneration and necrosis. Both CHA and epinephrine treatments alleviated these injuries, as reflected by reduced liver and kidney injury scores (Figs. 2I and J).
Figure 2
Figure 2.
CHA induced torpor-like status decreases the mortality of HS and inhibits the energy mobilization in liver. (A) Schematic of the experimental protocol. (B) Survival rate over 24 h following HS and treatment. (C) Core temperature over 5 h after HS and treatment. Cardiovascular parameters were analyzed among groups, including heart rate (D), respiratory rate (E), systolic pressure (F) and diastolic pressure (G). Histopathological analysis of liver and kidney tissues (H) and injury scores (I, J). Data are presented as mean ± SEM (n = 6 per group). One-way ANOVA followed by Tukey’s post hoc analysis was performed in all experiments. *P < 0.05 vs. Sham group; #P < 0.05 vs. HS group; $P < 0.05 vs. HS+CHA group. Scale bar: 100 µm. E, epinephrine.
The protective effect of CHA was also reflected by serum parameters (Table S1 in Supporting information). The ALT and AST levels were significantly elevated in the HS and epinephrine group. CHA treatment partially mitigated this increase, though the reduction did not reach statistical significance. TP and ALB were both significantly reduced in the HS group compared to Sham. CHA treatment led to further reduction in TP and ALB, which may indicate lower anabolic states. The HS and epinephrine group showed a dramatic elevation in CK levels, a marker of muscle damage, and reduced by CHA treatment. BUN levels were elevated in HS group and were not changed upon CHA or epinephrine treatment. CREA levels were slightly higher in the CHA group compared to HS group, suggesting possible kidney stress. LDH levels were significantly increased in the HS and epinephrine group but decreased by CHA treatment, indicating a different energy metabolism profile upon CHA treatment. Cholesterol and triglyceride levels were reduced in the HS group compared to Sham, which may indicate altered lipid metabolism as a result of HS. Neither CHA nor epinephrine seems to significantly improve lipid levels. Electrolyte balance was not severely affected by the treatments in the short term, though CHA may have a slight effect on chloride levels (Table S1).
Given that hypothermia typically disrupts normal coagulation processes [18], we evaluated the risk of coagulopathy with CHA treatment. Serum coagulation parameters were also evaluated (Table 1). No significant differences were observed in prothrombin time (PT) and thrombin time (TT) among the groups. HS group exhibited significant coagulation abnormalities compared to the Sham group, with a prolonged activated partial thromboplastin time (APTT) and elevated fibrinogen (FIB) levels. In the HS+CHA group, the APTT was even more prolonged than in the HS group, and fibrin degradation product (FDP) levels were significantly decreased compared to the HS group. Additionally, D-Dimer levels were higher in the HS+CHA group relative to the HS group. These changes suggest that CHA may exert an anticoagulant effect, influencing both the coagulation and fibrinolytic systems, and potentially mitigating hypercoagulable states caused by HS. We hypothesize that this may be linked to adenosine signaling in platelets and endothelial cells. Studies have shown that activation of adenosine 2A receptors significantly inhibits platelet aggregation by elevating intracellular cyclic adenosine monophosphate levels [19-21]. The role of A1 receptors, however, remains controversial. Furthermore, adenosine A1 receptor (A1AR) expression on endothelial cells is crucial for maintaining endothelial barrier function and microvascular permeability [22]. Whether these mechanisms contribute to coagulation processes warrants further investigation.
Table 1
Table 1.
Serum coagulation parameters of animals 2 h after HS.
Note: P value was determined by one-way ANOWA and multiple comparisons. *: vs. sham; #: vs. HS; $: vs. HS-CHA.
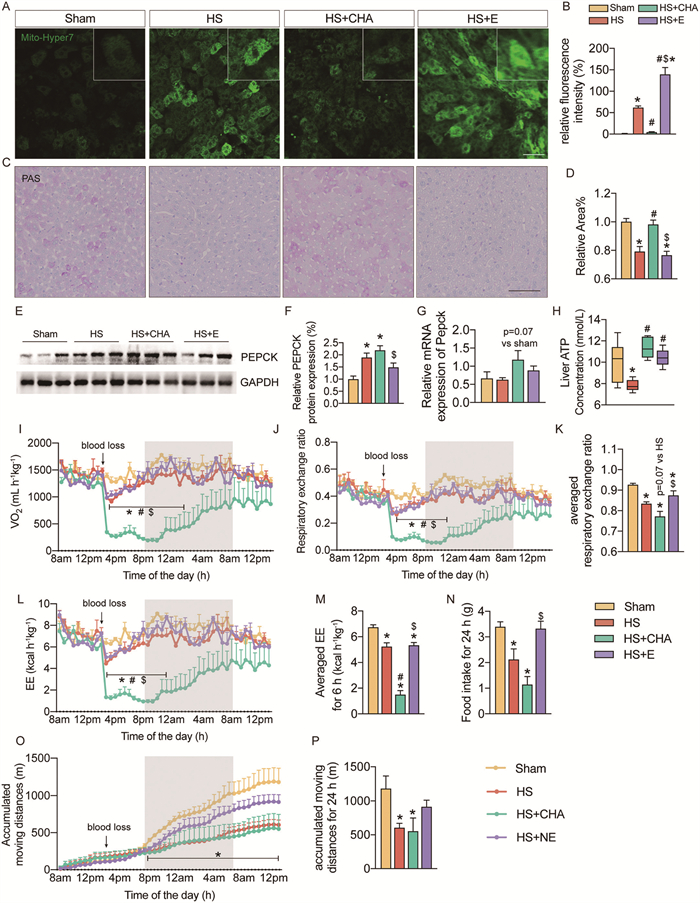
We next explored the mechanism from the metabolic aspect in major organs. Mitochondrial oxidative stress in the liver was assessed using the Mito-Hyper 7 probes [23]. Reactive oxygen species (ROS) production was significantly elevated in both the HS and HS+E groups, while it was markedly reduced in the HS+CHA group, indicating that CHA effectively suppressed mitochondrial activity and ROS generation (Figs. 3A and B). Additionally, we examined sympathetic nerve activity by quantifying Fos proto-oncogene (c-FOS)-positive neurons in the rostral ventrolateral medulla (RVLM) and locus coeruleus, regions closely associated with sympathetic output. We found that these nuclei were activated in the HS and HS+E groups, as expected, but inhibited in the HS+CHA group (Figs. S3A–C in Supporting information). This is consistent with the mitochondrial activity observed in the liver (Fig. 3A). PAS staining revealed significant glycogen depletion in the HS and HS+E groups, while CHA preserved glycogen levels (Figs. 3C and D). We further examined the expression of the key gluconeogenesis enzyme, phosphoenolpyruvate carboxykinase (PEPCK). Compared to the sham group, PEPCK protein levels were significantly elevated in both the HS and HS+CHA groups (Figs. 3E and F). PEPCK mRNA expression also has a trend to increase in HS+CHA group, although not statistically significant (Fig. 3G). Finally, we measured total hepatic ATP levels, which were significantly reduced in the HS group but restored in both the CHA and epinephrine groups (Fig. 3H). The whole-body metabolic activity was evaluated by metabolic cages. CHA administration significantly reduced metabolic rate during HS. Oxygen consumption was markedly decreased in the HS+CHA group (Fig. 3I). The respiratory exchange ratio (RER) was significantly lower in the HS+CHA group during the 6-h period following hemorrhage (Figs. 3J and K). Energy expenditure (EE) also showed a significant reduction in the HS+CHA group compared to both the HS and Sham groups, as shown by the averaged EE over 6 h post-HS (Figs. 3L and M). Moreover, food intake and physical activity was also significantly decreased in the HS+CHA group relative to the Sham group (Figs. 3N–P). Thus, CHA reduces mitochondrial ROS production and inhibits sympathetic nerve activation, which leads to decreased metabolic demand and protection of major organs in the HS mode.
Figure 3
Figure 3.
CHA decreases the metabolic rate in HS model. (A) Representative images of mitochondrial ROS levels in liver by Mito-Hyper7 probe. (B) Quantification of relative fluorescence intensity of Mito-Hyper7 in A. (C) Representative images of glycogen content in liver by periodic acid-Schiff (PAS) staining. (D) Quantification of relative glycogen area in C. (E) Western blot analysis showing protein expression levels of phosphoenolpyruvate carboxykinase (PEPCK) and glyceraldehyde-3-phosphate dehydrogenase (GAPDH) in liver. (F) Quantification of E. (G) Relative mRNA expression of PEPCK in liver. (H) ATP concentration in liver tissue lysate. (I) Oxygen consumption over time in four groups. (J, K) RER over time (J) and average RER during a 6-h period after HS (K). EE over time (L) and averaged energy expenditure during a 6-h period after HS (M). (N) Food intake over 24 h after HS. (O, P) Accumulated moving distances over time. Data are presented as mean ± SEM (n = 6 per group). One-way ANOVA followed by Tukey’s post hoc analysis was performed in K, M, N, P. Two-way ANOVA was performed for I, J, L, O to evaluate the effects of treatment and time on each parameter. Tukey’s post hoc test was conducted for multiple comparisons among the groups. *P < 0.05 vs. sham group; #P < 0.05 vs. HS group; $P < 0.05 vs. HS+CHA group. Scale bar: 50 µm for A, 20 µm for C.
First-line treatments for HS focus on rapid resuscitation, volume replacement, and restoring tissue perfusion [24]. However, in out-of-hospital settings, such as on the battlefield, these interventions are often delayed, making drugs that can extend the time window for medical evacuation crucial for HS management. In our study, we compared CHA with epinephrine, as they represent two completely opposite treatment strategies. Epinephrine increases blood pressure by acting as a potent vasoconstrictor, helping maintain tissue perfusion during acute hypotension. Hemorrhagic triggers hypercatabolism, and epinephrine mobilizes the body’s energy further in response to injury, which can lead to various side effects during later recovery stages. Therefore, epinephrine should be used transiently and with caution, as prolonged or high-dose use may increase cardiac workload and result in arrhythmias [25,26]. In contrast, CHA protects organs by reducing metabolic demand, with better survival rate than the epinephrine group. Tissue-level analysis revealed that oxidative stress and damage scores in the liver and kidney were also lower in the CHA group compared to epinephrine. These findings suggest CHA reduces hepatic energy consumption, activates gluconeogenesis, mitigates oxidative stress, and decreases organ damage in HS.
CHA treatment significantly altered the metabolic profile in the HS model, as revealed by metabolomics analysis. Orthogonal Partial Least Squares Discriminant Analysis (OPLS-DA) score plots demonstrated a clear separation of metabolic profiles between the Sham, HS, and HS+CHA groups in both positive and negative ion modes (Fig. S4A in Supporting information). Pathway enrichment analysis further identified key metabolic pathways affected by CHA treatment. Notably, the HS+CHA group showed significant enrichment in pathways involved in fatty acid biosynthesis, arginine biosynthesis, alanine, aspartate, and glutamate metabolism, as well as the tricarboxylic acid (TCA) cycle (Fig. S4B in Supporting information). These findings suggest that CHA influences both energy metabolism, lipid metabolism and amino acid metabolism during the HS.
Specific metabolites involved in key metabolic pathways were also significantly altered following CHA treatment. In the HS+CHA group, levels of several unsaturated fatty acids, including stearic acid, palmitic acid, and oleic acid, were increased compared to the HS group (Fig. S4C in Supporting information). Furthermore, glutathione metabolism was enhanced by CHA, as evidenced by increased levels of reduced glutathione and decreased levels of pyroglutamic acid. Cystine, leucine, and arginine were elevated in the HS group and reduced in the HS+CHA group. This may due to enhanced protein breakdown or increased amino acid mobilization for energy production under hemorrhagic stress, followed by a reduction in amino acid metabolism or a shift away from amino acid catabolism as the body conserves these resources during the torpor-like state induced by CHA. This pattern partially resembles metabolic adaptations observed during cold exposure. However, there are notable differences between the metabolic regulation in a hibernation-like state and cold exposure [27,28]. In cold exposure scenarios, the body remains in an energy mobilization state to maintain core body temperature, with increased energy demands, activation of the sympathetic nervous system, and enhanced heat production, thus burning fat. In contrast, in a hibernation-like state, the core body temperature decreases, energy demands are reduced, the sympathetic nervous system is not activated, and the increase in fat metabolism may stem from a controlled metabolic adaptation towards energy storage. In terms of glucose metabolism, both gluconeogenesis and glycogenolysis were more active under HS conditions, as expected [29]. CHA treatment, on the one hand, suppressed glycogenolysis, indicating a low-energy demand of body, while promoting gluconeogenesis, possibly linked to A1AR receptor signaling, which is known to stimulate hepatic gluconeogenesis [30,31]. Together, these results suggest that CHA treatment induces a shift towards enhanced fatty acid metabolism and improved antioxidant capacity, which may contribute to the protective effects of CHA in the HS model.
In conclusion, we successfully developed a stable CHA nasal gel that enhances brain delivery and effectively induces torpor-like hypothermia. Intranasal administration of CHA resulted in higher concentrations in the brain compared to intravenous delivery, leading to a more pronounced hypothermic response. This targeted approach significantly improved survival rates in a mouse model of HS, reduced metabolic rate, and minimized organ damage. This approach opens new avenues for further research into hypothermia-induced protection in critical care settings, as it facilitates rapid, non-invasive cooling, aligning with the need for quick deployment in emergency settings like military combat or remote areas. To scale up the CHA nasal gel for clinical use, potential challenges include the need for consistent storage conditions to maintain the integrity of the nasal gel, especially in resource-limited settings. Strategies such as stabilizing agents or improved packaging can be explored to address these challenges.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
CRediT authorship contribution statement
Chunlei Hui: Writing – original draft, Visualization, Validation, Investigation, Formal analysis, Data curation, Conceptualization. Xiuqing Li: Software, Investigation, Formal analysis, Data curation. Ying Liang: Validation, Software, Methodology, Data curation. Qingqiu Huang: Validation, Investigation. Li Fan: Project administration, Conceptualization. Li Su: Writing – review & editing, Supervision, Project administration, Funding acquisition. Yuanqing Gao: Writing – review & editing, Writing – original draft, Visualization, Supervision, Methodology, Funding acquisition, Conceptualization.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (No. 81981340417 to Li Su), and Natural Science Foundation of Jiangsu Province Outstanding Youth Fund (No. BK20240134 to Yuanqing Gao).
Supplementary materials
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.cclet.2025.111017.
I. Faria, N. Thivalapill, J. Makin, et al., Crit. Care Clin. 38 (2022) 775–793. doi: 10.1016/j.ccc.2022.06.013
[4]
A. Sauaia, E.E. Moore, C.E. Wade, J.B. Holcomb, Epidemiology of hemorrhage-related mortality, in: H.B. Moore, M.D. Neal, E.E. Moore (Eds.), Trauma Induced Coagulopathy, Springer International Publishing, Cham, 2021, pp. 13–27.
M. Amor, M. Diaz, V. Bianco, et al., Cardiovasc. Diabetol. 23 (2024) 298. doi: 10.1186/s12933-024-02397-7
[29]
A. D’Alessandro, H.B. Moore, E.E. Moore, et al., Am. J. Physiol. Regul. Integr. Comp. Physiol. 308 (2015) R1034–R1044. doi: 10.1152/ajpregu.00030.2015
[30]
S. Jain, L.F. Barella, J. Wess, et al., Biochem. Pharmacol. 192 (2021) 114739. doi: 10.1016/j.bcp.2021.114739
[31]
L. Antonioli, C. Blandizzi, B. Csóka, et al., Nat. Rev. Endocrinol. 11 (2015) 228–241. doi: 10.1038/nrendo.2015.10
Figure 1
Preparation of a CHA nasal gel and its distribution dynamics. (A) The procedure of the preparation of CHA nasal gel. (B) Timeline of CHA administration intranasally (i.n.) or intravenously (i.v.) at a dose of 1.5 mg/kg. Blood and tissue samples were collected at various time points post-administration for analysis. (C) Stability test of CHA in the nasal gel formulation over 8 weeks. Concentration of CHA in plasma (D), heart (E), whole brain (F) and hypothalamus (G) over time following CHA administration. (H) Core temperature changes over time following CHA administration. Data are presented as mean ± SEM. Unpaired t-test was performed in all experiments. *P < 0.05.
Figure 2
CHA induced torpor-like status decreases the mortality of HS and inhibits the energy mobilization in liver. (A) Schematic of the experimental protocol. (B) Survival rate over 24 h following HS and treatment. (C) Core temperature over 5 h after HS and treatment. Cardiovascular parameters were analyzed among groups, including heart rate (D), respiratory rate (E), systolic pressure (F) and diastolic pressure (G). Histopathological analysis of liver and kidney tissues (H) and injury scores (I, J). Data are presented as mean ± SEM (n = 6 per group). One-way ANOVA followed by Tukey’s post hoc analysis was performed in all experiments. *P < 0.05 vs. Sham group; #P < 0.05 vs. HS group; $P < 0.05 vs. HS+CHA group. Scale bar: 100 µm. E, epinephrine.
Figure 3
CHA decreases the metabolic rate in HS model. (A) Representative images of mitochondrial ROS levels in liver by Mito-Hyper7 probe. (B) Quantification of relative fluorescence intensity of Mito-Hyper7 in A. (C) Representative images of glycogen content in liver by periodic acid-Schiff (PAS) staining. (D) Quantification of relative glycogen area in C. (E) Western blot analysis showing protein expression levels of phosphoenolpyruvate carboxykinase (PEPCK) and glyceraldehyde-3-phosphate dehydrogenase (GAPDH) in liver. (F) Quantification of E. (G) Relative mRNA expression of PEPCK in liver. (H) ATP concentration in liver tissue lysate. (I) Oxygen consumption over time in four groups. (J, K) RER over time (J) and average RER during a 6-h period after HS (K). EE over time (L) and averaged energy expenditure during a 6-h period after HS (M). (N) Food intake over 24 h after HS. (O, P) Accumulated moving distances over time. Data are presented as mean ± SEM (n = 6 per group). One-way ANOVA followed by Tukey’s post hoc analysis was performed in K, M, N, P. Two-way ANOVA was performed for I, J, L, O to evaluate the effects of treatment and time on each parameter. Tukey’s post hoc test was conducted for multiple comparisons among the groups. *P < 0.05 vs. sham group; #P < 0.05 vs. HS group; $P < 0.05 vs. HS+CHA group. Scale bar: 50 µm for A, 20 µm for C.

 DownLoad:
DownLoad:

 下载:
下载:




