Figure 1.
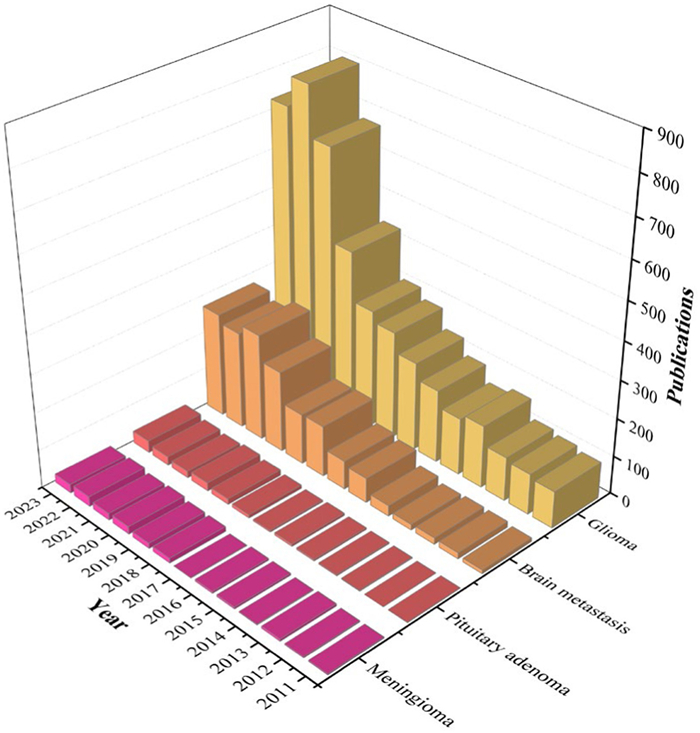
Annual publication trends in immunotherapy for brain metastasis, glioma, meningioma, and pituitary adenoma.
Knowledge structures and research hotspots of immunotherapy for brain metastasis, glioma, meningioma, and pituitary adenoma: A bibliometric and visualization review
Donghu Yu , Junneng Wang , Lei Hu , Youxian Wu , Tianqing Wang , Zhiyu Li , Zefen Wang , Qihang Ding , Yao Sun , Zhiqiang Li

Cancer immunotherapy is an innovative treatment method that leverages the patient's adaptive and innate immune responses to combat tumors [1,2]. Various immunotherapeutic strategies have demonstrated promising outcomes in enhancing prognosis and life expectancy in non-brain cancers [3–6]. Immunotherapy has been explored as a treatment for brain tumors; however, progress in this area has been limited. The unique microenvironment of brain tumors presents significant biological challenges that hinder the effectiveness of immunotherapeutic approaches. The blood-brain barrier restricts the delivery of therapeutic agents and impedes the infiltration of immune cells [7–9]. Additionally, brain tumors exhibit considerable genetic and phenotypic heterogeneity, resulting in variable responses to immunotherapeutic agents [10]. Nonetheless, recent findings regarding the effectiveness of immunotherapy in brain metastases offer valuable insights into the immunobiology of brain tumors, providing important clues for the development of immunotherapeutic drugs targeting primary brain tumors.
Brain metastasis is the most prevalent form of intracranial malignancy in adults, occurring 10 times more frequently than primary intracranial neoplasms [11–13]. Immunotherapy, both alone and in combination with conventional treatments, has been effective in combating the spread of brain metastasis and reducing tumor burden [13–15]. Glioma is the most prevalent primary brain tumor. Glioblastoma multiforme (GBM) is the most aggressive of the glioma, which responds poorly to traditional treatments typically [16,17]. Immunotherapy is evolving as a promising approach to treating GBM, and recent clinical trials have shown that neoadjuvant anti-programmed death protein-1 (PD-1) immunotherapy improves intratumoral immune responses in recurrent glioblastoma [18,19]. Meningiomas, which account for approximately one-third of diagnosed central nervous system (CNS) tumor each year, are classified into grades 1–3 by the World Health Organization (WHO) [20]. High-grade meningiomas (grades 2 and 3) account for approximately 18% of cases and display more aggressive characteristics. Conventional treatment options have proven ineffective in enhancing progression-free survival for these tumors [20,21]. Consequently, alternative strategies, such as chimeric antigen receptor (CAR) T cell and immune checkpoint inhibitors (ICIs), are being explored to engage the immune system against them [22,23]. Pituitary tumors, accounting for approximately 10%–15% of brain tumors, are the second most prevalent type of primary brain tumor in humans [24,25]. While most pituitary tumors grow slowly and are non-invasive, around 10% exhibit aggressive behavior and resist standard therapies. Preclinical studies indicate that aggressive pituitary adenomas have elevated levels of programmed death-ligand 1 (PD-L1) and tumor-infiltrating lymphocytes (TILs), suggesting that PD-1 blockade may offer a promising therapeutic strategy [26,27]. Overall, these new discoveries underscore the significant potential of immunotherapy in the treatment of various brain tumors, including brain metastases, gliomas, meningiomas and pituitary adenomas. However, there is a lack of comprehensive reporting on publication trends, institutional collaborations, trial distribution, and immunotherapy drugs hotspots for these specific tumor types.
This study aims to fill the research gap by examining systematically the research on immunotherapy drugs for brain metastasis, glioma, meningioma, and pituitary adenoma. A comprehensive bibliometric analysis is performed to evaluate the scientific production of immunotherapy research in brain tumors, characterize immunotherapy research activities, and identify patterns, tendencies, and regularities of immunotherapy-related articles for different intracranial tumors. This analysis helps to assess global collaboration patterns between authors, institutions and countries, identify research trends and uncover hotspots in these areas.
Relevant publications were downloaded from the Web of Science Core Collection (WoSCC). WoSCC is a comprehensive database for scientific research containing over 12,000 high-quality journals. Previous studies have confirmed that WoSCC is well-suited for conducting bibliometric analysis [28–31]. Based on a review of the literature, we identified common keywords related to immunotherapy, brain metastasis, glioma, meningioma, and pituitary adenoma. We developed search formulas for each area by intersecting these keywords (Table S1 in Supporting information). Only English-language articles or reviews published between January 1, 2011, and December 31, 2023, were included. 6084 publications were selected (immunotherapy for brain metastasis: 1520 papers; immunotherapy for glioma: 4302 papers; immunotherapy for meningioma: 120 papers; immunotherapy for pituitary adenoma: 142 publications) (Fig. S1 in Supporting information).
General information about the publications—such as publication dates, journals, authors' institutions, and keywords—was analyzed using the "bibliometrix" package in R software [32]. The scientific collaboration networks for countries, institutions, and researchers, were further visualized by "bibliometrix" package. Besides, VOSviewer software [33] was employed to examine trends in country cooperation, co-citation references, and keyword frequencies over time.
The number of publications concerning immunotherapy for brain tumors increased yearly (Fig. 1). In immunotherapy for brain metastasis, publication outputs remained low between 2011 and 2015. From 2016 to 2021, the volume of literatures has steadily increased, indicating that immunotherapy has attracted growing attention in the therapy research for brain metastasis. From 2021 to 2023, the number of publications remained stable. For glioma immunotherapy, the scientific publication output kept steady and rapid growth every year, and immunotherapy as a promising treatment for glioma has caused wide attention. In contrast, immunotherapeutic research in meningiomas and pituitary adenomas was still at a very early stage and the overall research trends in these areas cannot be adequately represented.
A total of 1822 institutions from 60 countries have published 1520 articles on the immunotherapy for brain metastasis; 4302 articles on glioma immunotherapy were published by 2841 organizations from 84 countries; 283 institutions from 23 countries published 120 articles on immunotherapy for meningiomas; 308 institutions from 23 countries published 142 articles on immunotherapy for pituitary adenomas. The United States of America (USA) and China published many important papers. The USA held the top position of total citations in immunotherapy for brain metastasis, glioma, meningioma, and pituitary adenoma, with 16,641, 60,351, 969, and 893 citations, respectively (Table S2 in Supporting information). China, while ranking second globally in the volume of publications on immunotherapy for brain metastasis and glioma, had one of the lowest citation averages per article among the top ten countries. The majority of the leading institutions in terms of publication counts were based in the USA, with the University of Texas MD Anderson Cancer Center holding the top position in both publication output and citation impact in this field (Table S3 in Supporting information). Harvard Medical School led in the number of publications on immunotherapy of gliomas and meningiomas. Capital Medical University (China) was the most active in the immunotherapy of pituitary adenomas. The analysis of the collaboration network revealed that scientific cooperation between countries is mainly focused on US-China cooperation (Fig. S2 in Supporting information).
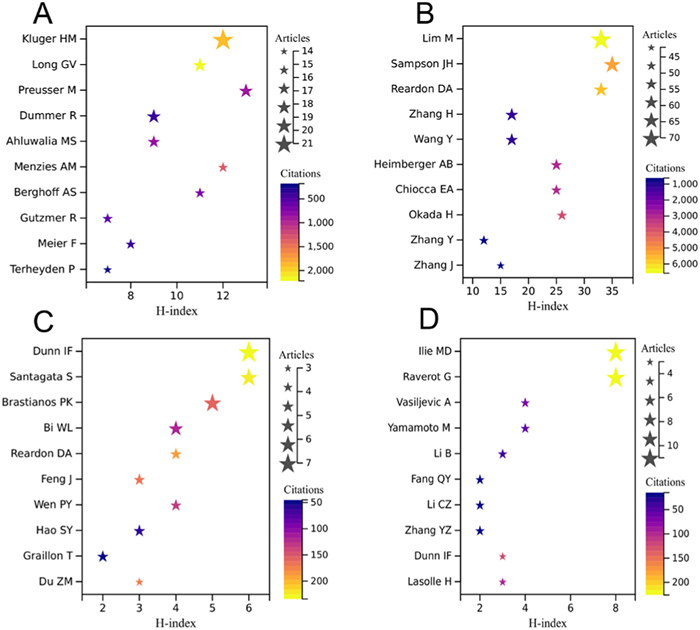
A total of 9463, 20,413, 891, and 829 researchers have contributed to immunotherapy-related papers for brain metastasis, glioma, meningioma, and pituitary adenoma, respectively. In immunotherapy for brain metastasis, Kluger ranked first in publication outputs with 21 papers, followed by Long, Preusser, and Dummer (each with 17 papers). Lim (70 papers) was found to be the most productive author for glioma immunotherapy, followed by Sampson (61 papers) and Reardon (55 papers). There were relatively few research articles for meningioma immunotherapy, and Dunn had the highest number of papers (7 papers). In immunotherapy for pituitary adenoma, Raverot and Ilie shared first place with 11 papers each (Table S4 in Supporting information).
Long was the most cited author (2216 citations) in the field of immunotherapy for brain metastasis, followed by Kluger (1927 citations) and Menzies (1346 citations). For glioma immunotherapy, three authors had been cited over 5000 times, with Lim being the most cited author (6583 citations), followed by Reardon (5805 citations) and Sampson (5338 citations). Dunn had the highest number of citations (234 citations) for meningioma immunotherapy, followed by Santagata (229 citations). The field of immunotherapy for pituitary adenoma was still in its infancy, and only three authors (Ilie, 226 citations; Raverot, 226 citations; Dunn, 126 citations) had been cited more than 100 times so far (Table S4). For the H-index score, the gaps between the top 10 productive authors in each area were insignificant. However, as widespread attention to glioma immunotherapy grew, the H-index scores of researchers were much higher than those of the researchers in the other three areas (Fig. 2). The network analysis of the co-researchers also revealed a worrying lack of collaboration at a global level, particularly in the immunotherapy of meningiomas and pituitary adenomas (Fig. S3 in Supporting information).
The journal "Frontiers in Oncology" had the highest number of outputs in the fields of immunotherapy for brain metastasis (82 articles), followed by "Cancers" (62 articles) and "The Journal for ImmunoTherapy of Cancer" (46 articles). In the field of glioma immunotherapy, "Frontiers in Immunology" had the highest number of publications with 222 articles, followed by "Frontiers in Oncology" (167 articles) and "Cancers" (137 articles). For meningioma immunotherapy, the journals "Frontiers in Endocrinology" and "Journal of Neuro-Oncology" had the highest number of outputs with 9 articles each. The journal "Frontiers in Endocrinology" was a highly-yield journal in immunotherapy for pituitary adenoma with 11 publications. Among the top 10 academic journals publishing the most articles, more than half of the journals belonged to Journal Citation Reports Quartile in Category 1 (Table S5 in Supporting information).
In the field of immunotherapy for brain metastasis, the journal "Journal of Clinical Oncology" had the most local citations, followed by "The New England Journal of Medicine". The journal "NQ1euro-Oncology" was most frequently cited for glioma immunotherapy and meningioma immunotherapy, and the journal "The Journal of Clinical Endocrinology & Metabolism" had the highest number of citations (432 times) in immunotherapy for pituitary adenoma (Fig. S4 in Supporting information).
In the field of immunotherapy for brain metastasis, "Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: early analysis of a non-randomized, open-label, phase 2 trial" [34] is the most locally cited paper (257 times). For glioma immunotherapy, the article with the highest number of citations was "Regression of Glioblastoma after Chimeric Antigen Receptor T-Cell Therapy" [35], cited 372 times locally. The paper titled "Expression and prognostic impact of immune modulatory molecule PD-L1 in meningioma" [36] had the highest number of citations in meningioma immunotherapy, and "Increased expression of PD-L1 in human pituitary tumors" [27] ranked first in local citations in the fields of immunotherapy for pituitary adenoma (Table S6 in Supporting information).
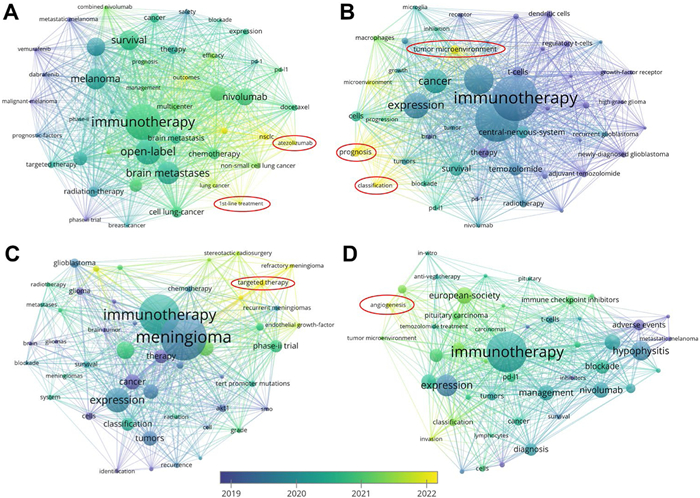
Through further visualizing text analysis results with temporal distribution of keywords (Fig. 3), we found that the keywords "1st-line treatment" and "atezolizumb" are moving into the center from the margin in immunotherapy for brain metastasis currently. For glioma immunotherapy, "prognosis, " "classification, " and "tumor microenvironment" have become more important. "Targeted therapy" and "angiogenesis" are popular keywords in immunotherapy for meningioma and pituitary adenoma, respectively.
In the last decade, groundbreaking discoveries have elucidated the anatomy, genetics and function of the immune system in the central nervous system [37–39], leading to the moral development of immunotherapy for brain metastases, gliomas, meningiomas, and pituitary adenomas. We first analyzed the contributions of countries and institutions to immunotherapy research for brain tumors. The USA and China ranked among the top two countries in terms of the number of publications, indicating their leading roles in immunotherapy-related research on brain tumors. Besides, a majority of the top 10 organizations with the highest publications were from the USA, which suggested that American institutions currently play an international leading role. However, the distribution of organizations was dispersed, with no clear network forming among the primary research targets. Some researchers even lacked connections with others, suggesting a deficiency in academic communication among these institutions. This situation would inevitably hamper the development of related areas of study, particularly on the immunotherapy for meningiomas and pituitary adenomas. To our knowledge, it is the first time to perform comprehensive bibliometric analysis on immunotherapy for various brain tumors. One of the main purposes of the comprehensive analysis is to compare the developing tendencies, research hotspots, and frontiers between different fields. The groundbreaking research in a certain filed would provide useful reference for others. Particularly, the fluctuating developmental process in glioma immunotherapy would offer reference for the research on immunotherapy for meningioma and pituitary adenoma, which is still in early stages.
From 2011 to 2015, the limited publication outputs suggested that immunotherapy-related research for brain metastasis was at the initial stage. In 2016, a groundbreaking study by Kluger et al. (NCT02085070) accelerated the development of this field, reporting the clinical benefits of pembrolizumab on patients with melanoma or non-small cell lung cancer (NSCLC) brain metastases [34]. Subsequently, the publications on this topic had grown, and some remarkable achievements have been made from 2017 to 2022. For example, in 2018, Tawbi et al. conducted a multicenter randomized phase 2 study, demonstrating that nivolumab combined with ipilimumab were effective in melanoma brain metastases, and they proposed that nivolumab in combination with ipilimumab should be considered a first-line treatment for patients with asymptomatic untreated brain metastases [40]. In the immunotherapy domain for brain metastasis, Kluger emerged as the leading researcher with 21 publications. As mentioned above, Kluger's team identified the short-term efficacy of pembrolizumab in melanoma brain metastases (NCT02085070) in 2016, and the paper "Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: Early analysis of a non-randomized, open-label, phase 2 trial" [34] had the highest number of local citations. In 2019, further research by his team demonstrated that two-year survival was similar to patients without brain metastasis treated with pembrolizumab, and they suggested that pembrolizumab should be used to treat small, asymptomatic brain metastases [41]. In general, the researchers focused more on the clinical application of ICIs in immunotherapy for brain metastasis.
Though several works have already conducted bibliometric analyses of glioma immunotherapy [42,43], the inaccurate search strategy downgraded the research quality of these bibliometric studies. Therefore, more efforts should be made to provide more accurate data to analyze the research trends of immunotherapy for glioma. In this study, we found that the number of publications on glioma immunotherapy has increased yearly. In 2019, two randomized clinical trials showed that neoadjuvant anti-PD-1 immunotherapy promotes intratumoral responses in recurrent glioblastoma [18,19], which propelled the research and development of glioma immunotherapy, leading to an explosion of publications from 2020 to 2023. For glioma immunotherapy, Lim ranked first with the highest number of publications (70 articles), followed by Sampson (61 articles), and Reardon (55 articles). Lim's review "Current state of immunotherapy for glioblastoma" [44] described the state of immunotherapy for gliomas (notably glioblastoma) and the future directions for glioma immuno-oncology, which got high citations. In 2020, Reardon's team reported that nivolumab monotherapy did not enhance overall survival (OS) compared to bevacizumab in the treatment of recurrent glioblastoma (NCT02017717), and the paper "Effect of nivolumab vs. bevacizumab in patients with recurrent glioblastoma" [45] was highly cited. The papers, top two in terms of local citations, titled "Regression of glioblastoma after chimeric antigen receptor T-cell therapy" [35] and "A single dose of peripherally infused EGFRvIII-directed CAR T cells mediates antigen loss and induces adaptive resistance in patients with recurrent glioblastoma" [46] provided initial evidence for the anti-tumor efficacy and safety of CAR-T in glioma patients. Considering the publication time of highly cited papers, we found that the popular direction has shifted from CAR-T therapy to ICI treatment for glioma, especially after confirming that the neoadjuvant administration of PD-1 inhibitor promoted a survival benefit in recurrent glioblastoma [18]. Some highly-cited journals focused on glioma immunotherapy primarily publish articles related to new nanomaterials. This trend indicates a significant development of nanomaterials aimed at enhancing glioma immunotherapy. There have been certain nanomaterials developed to induce immunogenic cell death (ICD) to improve glioma immunotherapy [47–50]. By triggering the release of damage-associated molecular patterns, ICD stimulates the activation and maturation of dendritic cells, which leads to the presentation of tumor antigens and the subsequent mobilization of T cells [51,52]. The combination of ICI treatment with advanced nanotechnology represents a promising trend in the future of glioma therapy.
In contrast, research on immunotherapy for meningioma and pituitary adenoma was still in the development phase and should be investigated in more detail in the future. Historically, funding for brain tumor research has been disproportionately allocated to more common malignancies, such as gliomas, due to their higher mortality rates and public awareness. Meningiomas and pituitary adenomas, which are often less aggressive and have better prognosis, may receive less focus and fewer financial resources. This lack of funding can hinder the advancement of novel research initiatives and affect the scope of clinical trials. Dunn published many important papers regarding the immunotherapy for meningiomas, with 7 articles. Reardon and his team first performed a phase 2 study of nivolumab among patients with grade ≥2 meningiomas that recurred after surgery and radiation therapy (NCT02648997) [53]. The article "Expression and prognostic impact of immune modulatory molecule PD-L1 in meningioma" by Han et al. [36] emerged as the most locally cited paper. The paper analyzed the association between PD-L1 expression and survival outcomes in high grades meningiomas, which suggested that ICIs could be clinically effective for meningiomas that overexpress PD-L1. In immunotherapy for pituitary adenoma, Raverot and Ilie tied for first place with 11 published papers each. Raverot and Ilie were in the same research team. As a pioneer of immunotherapy for pituitary adenoma, Raverot' team first reported the real-world efficacy of ICIs in pituitary carcinomas and aggressive pituitary tumors [54]. The article with the highest number of local citations, titled "Increased expression of PD-L1 in human pituitary tumors" by Mei et al. [27], identified that pituitary adenomas harbored PD-L1 across subtypes, suggesting that the existence of an immune response to pituitary tumors and the possibility of considering ICIs in cases refractory to conventional management.
We also focus on new clinical evidence for the efficacy of immunotherapy in brain tumors and the implications of these findings for daily practice. By summarizing the active clinical trials, which are currently recruiting patients, we can clarify the frontiers and prospects of immunotherapy for brain metastasis, glioma, meningioma, and pituitary adenoma.
The major immunotherapies currently under study encompass ICIs, CAR-T therapy, tumor vaccines, and oncolytic virus (OV) therapy (Fig. 4) [2,55–58]. ICIs function by obstructing the binding of checkpoint proteins to their partner proteins, thus empowering T cells to initiate tumor cell death. Notable targets for checkpoint proteins include PD-1 (nivolumab, pembrolizumab), PD-L1 (durvalumab, atezolizumab), and cytotoxic T-lymphocyte associated protein 4 (CTLA-4; ipilimumab) [59–61]. CAR-T therapy employs CAR technology, where synthetic receptors are affixed to T cells. By binding to the major histocompatibility complex, CAR-T cells gain the ability to identify and eliminate tumor cells [62–65]. Tumor vaccines exploit tumor-associated antigens that are either present at low levels or absent in healthy cells [57,66]. These vaccines prime the immune system to recognize and respond to these specific antigens, facilitating the targeting and eradication of cancer cells [67–69]. Oncolytic viral therapy involves the injection of viruses into tumors, and these viruses infect both neighboring normal tissue and cancer cells. While normal cells efficiently clear the virus, cancer cells are incapable of doing so. As a result, the virus proliferates uncontrollably within the cancer cells, ultimately leading to their demise [70–72].

Brain metastasis is the prevailing form of brain tumors. Historically, a diagnosis of brain metastasis has been synonymous with a dire prognosis [73–75]. In recent years, immunotherapy, either as a stand-alone approach or in conjunction with conventional treatments, has proven to be a formidable force in the fight against the spread of brain metastases and in reducing the tumor size. Previous studies have focused on the efficacy of immunotherapy as a monotherapy, and the research results preliminarily proved its clinical benefit [11,76–79]. ICIs have established their position in metastatic NSCLC, as outlined by the National Comprehensive Cancer Network guidelines. However, due to tumor heterogeneity, the response to monotherapies varies. Therefore, it is crucial to address these tumors using a combination of two or more therapeutic approaches. These may include chemo-immunotherapies or radiotherapy combined with immunotherapy. Most studies have focused on directly comparing traditional radiotherapy with immunotherapy or a combination thereof. The addition of immunotherapy to stereotactic radiosurgery (SRS), a highly precise form of therapeutic radiation, has significantly improved median survival in patients with metastatic brain melanoma [80–84]. Moreover, several clinical trials for NSCLC patients with brain metastasis have shown that the combination of SRS with ICIs has led to reduced distant brain failure, decreased incidence of neurological brain death, and improved OS rates [85–88]. By contrast, the data comparing chemotherapy and chemo-immunotherapy were limited.
Investigating the impact of immunotherapy on brain metastasis patients receiving corticosteroids is an active and important area of research. A significant proportion of patients with brain metastasis require continuous corticosteroid treatment to manage symptoms related to the central nervous system [89]. However, the use of corticosteroids can suppress the systemic immune system, potentially affecting the efficacy of immunotherapy, which aims to enhance the immune response. A retrospective cohort study found that patients receiving both corticosteroids and immunotherapy had a four-month decrease in median survival compared to those who did not receive concurrent corticosteroid treatment, with the latter group experiencing an eight-month survival [89]. To obtain more conclusive results, an ongoing clinical trial (NCT03563729) (Table 1) is currently underway to ascertain whether the administration of ICIs provides clinical benefits for melanoma patients with brain metastases who are also receiving corticosteroids. Another case series explored the use of bevacizumab, a vascular endothelial growth factor inhibitor, as an alternative to corticosteroids in brain metastasis patients undergoing immunotherapy, aiming to determine if it reduced peritumoral edema without compromising the treatment effectiveness [90]. While bevacizumab appeared to prolong median survival compared to corticosteroids, concerns arose regarding the introduction of an additional agent that may increase the risk of bleeding, especially in patients with brain metastases who already have a heightened propensity for spontaneous bleeding unrelated to the bevacizumab treatment [90]. It is essential to conduct further in-depth research to address the significant therapeutic needs of patients receiving immunosuppressants.
 DownLoad:
CSV
DownLoad:
CSV
| Immunotherapy | Trial identifier | Study title | Study start | Phase |
| Pembrolizumab or combination of ipilimumab and nivolumab | NCT03563729 | Melanoma metastasized to the brain and steroids | 2018/6/6 | Phase 2 |
| CAR T cell | NCT03696030 | HER2-CAR T cells in treating patients with recurrent brain or leptomeningeal metastases | 2018/8/31 | Phase 1 |
| Combination of dendritic cell vaccines against Her2/Her3 and pembrolizumab | NCT04348747 | Dendritic cell vaccines against Her2/Her3 and pembrolizumab for the treatment of brain metastasis from triple negative breast cancer or HER2+ breast cancer | 2022/12/19 | Phase 2 |
Several ongoing clinical trials are advancing the application of immunotherapy in the context of brain metastasis. One such trial, NCT03696030, is a phase 1 study evaluating the effectiveness of intraventricular administration of HER2-CAR T-cells in the treatment of brain metastasis and leptomeningeal spread in recurrent cancer. Additionally, NCT04348747 focuses on investigating the use of dendritic cell vaccines targeting HER2/HER3, combined with the pembrolizumab treatment, specifically for patients with brain metastasis derived from triple-negative breast cancer or HER2+ breast cancer.
GBM is the most common and aggressive type of primary intrinsic glioma in adults, without isocitrate dehydrogenase mutations for targeted therapy [91–95]. Numerous immunotherapy clinical trials have been conducted for GBM patients, with 17 ongoing trials currently recruiting patients (Table 2). These trials explore various approaches such as ICIs, CAR-T cell therapy, tumor vaccines, and OV therapy. In recurrent GBM, it has been observed that administering a PD-1 inhibitor before tumor resection enhances local and systemic antitumor immune responses [18]. Consequently, ICIs targeting the PD-1/PD-L1 and CTLA-4 inhibitory pathways have become a focal point in research on GBM-induced immunosuppression. Several neoadjuvant therapy studies are currently in progress, primarily targeting recurrent gliomas (NCT04977375, NCT04656535). One notable combination is the use of domvanalimab (anti-TIGIT) alongside zimberelimab (anti-PD-1; NCT04656535). These agents may modulate T cells in the tumor environment or periphery [96–99]. In addition to ICIs, other approaches are being developed to overcome intratumoral heterogeneity and the immunosuppressive elements in the GBM microenvironment. CAR-T cell therapy, which has shown effectiveness in selected patients, is being expanded to target multiple antigens to account for GBM heterogeneity [100–102]. An ongoing clinical trial is currently investigating CAR-T cells targeting CXCR2 and CD70 (NCT05353530).
DownLoad:
CSV
| Immunotherapy | Trial identifier | Study title | Study start | Phase |
| Pembrolizumab | NCT04977375 | Trial of anti-PD-1 immunotherapy and stereotactic radiation in patients with recurrent glioblastoma | 2021/12/9 | Phase 1/2 |
| Pembrolizumab | NCT05235737 | The assessment of immune response in newly diagnosed glioblastoma patients treated with pembrolizumab | 2022/3/1 | Phase 4 |
| Daratumumab | NCT04922723 | Radiation/temozolomide and immunotherapy with daratumumab to improve antitumor efficacy in glioblastoma | 2022/10/3 | Phase 1/2 |
| Combination of AB154 and AB122 | NCT04656535 | AB154 combined with AB122 for recurrent glioblastoma | 2021/4/21 | Phase 1 |
| Combination of D2C7-IT and 2141-V11 | NCT05734560 | D2C7-IT and 2141-V11 in newly diagnosed GBM patients | 2023/9/6 | Phase 1/2 |
| CARv3-TEAM-E T cell | NCT05660369 | CARv3-TEAM-E T cells in glioblastoma | 2023/3/22 | Phase 1 |
| C7R-GD2.CAR T cell | NCT04099797 | C7R-GD2.CAR T cells for patients with GD2-expressing brain tumors | 2020/2/3 | Phase 1 |
| B7H3-specific CAR T cell | NCT04185038 | Study of B7-H3-Specific CAR T cell locoregional immunotherapy for diffuse intrinsic pontine glioma/diffuse midline glioma and recurrent or refractory pediatric central nervous system tumors | 2019/12/11 | Phase 1 |
| B7-H3, EGFR806, HER2, And IL13-Zetakine CAR T cell | NCT05768880 | Study of B7-H3, EGFR806, HER2, and IL13-zetakine (Quad) CAR T cell locoregional immunotherapy for pediatric diffuse intrinsic pontine glioma, diffuse midline glioma, and recurrent or refractory central nervous system tumors | 2023/5/5 | Phase 1 |
| CD70 CAR T cell | NCT05353530 | Phase I study of IL-8 receptor-modified CD70 CAR T cell therapy in CD70+ and MGMT-unmethylated adult glioblastoma (IMPACT) | 2023/7/25 | Phase 1 |
| TVI-Brain-1 | NCT05685004 | Study of neoantigen-specific adoptive T cell therapy for newly diagnosed MGMT negative GBM | 2023/9/15 | Phase 1/2 |
| H3K27M peptide vaccine | NCT04808245 | A multicenter phase Ⅰ peptide vaccine trial for the treatment of H3-mutated gliomas | 2023/2/15 | Phase 1 |
| TTRNA-xALT | NCT04837547 | PEACH TRIAL-precision medicine and adoptive cellular therapy | 2021/9/20 | Phase 1 |
| Dendritic cell vaccine | NCT04801147 | Immunotherapy with autologous tumor lysate-loaded dendritic cells in patients with newly diagnosed GBM | 2010/6/1 | Phase 1/2 |
| DOTAP liposome vaccine | NCT04573140 | A study of RNA-lipid particle (RNA-LP) vaccines for newly diagnosed pediatric high-grade gliomas (pHGG) and adult glioblastoma (GBM) | 2021/10/26 | Phase 1 |
| VBI-1901 | NCT03382977 | Study to evaluate safety, tolerability, and optimal dose of candidate GBM vaccine VBI-1901 in recurrent GBM subjects | 2017/12/6 | Phase 1/2 |
| rQNestin34.5v.2 | NCT03152318 | A study of the treatment of recurrent malignant glioma with rQNestin34.5v.2 | 2017/7/18 | Phase 1 |
Vaccination strategies against GBM have been investigated for many years, but previous approaches have struggled to address antigen expression heterogeneity and the expansion of T cells within tumors [103–105]. A new cancer vaccine, VBI-1901 (NCT03382977), has shown encouraging efficacy in treating recurrent GBM, effectively controlling disease progression in patients [106]. The United States Food and Drug Administration has awarded VBI-1901 both fast track designation and orphan drug designation for the treatment of recurrent GBM.
Furthermore, oncolytic viral therapy shows promise in addressing the complex tumor microenvironment [107]. OVs trigger pro-inflammatory changes in the microenvironment by delivering viral proteins and nucleic acids, as well as releasing danger signals through lysis and the subsequent release of GBM antigens [108,109]. Previous studies have demonstrated the anti-tumor effects and low neurotoxicity of the oncolytic herpes simplex virus (oHSV) treatment [109–112]. An ongoing trial (NCT03152318) aim to provide new insights and evidence for the promising use of oHSV in GBM.
Meningioma is a common type of CNS tumor, accounting for approximately one-third of diagnosed cases each year. The WHO classifies meningiomas into grades 1–3, with high grades (2 and 3) associated with increased growth rate, invasiveness, recurrence, and worse outcomes compared to grade 1 meningiomas [113,114]. Conventional treatments, including radiotherapy and chemotherapy, have shown limited effectiveness in improving survival for high-grade meningiomas [113,115]. Consequently, new treatment approaches are necessary to address these aggressive tumors. Extensive research has investigated the interaction between meningiomas and their immune landscape. Studies on the immune microenvironment of meningiomas reveal the expression of checkpoint molecules, including PD-L1, PD-L2, and CTLA-4, which may contribute to a partial suppression of anti-tumor immune responses [116–118]. Additionally, the absence of a blood-brain barrier permits the infiltration of immune cells such as T cells, B cells, macrophages, and plasma cells [119]. Moreover, the infiltrating immune population is largely composed of antigen-experienced T and B cells. Fang et al. further identified elevated levels of PD-1 and TIM-3, markers associated with T cell exhaustion [120]. Notably, in grade 3 meningiomas, there is a depletion of CD4 and CD8 T-cells alongside an increased proportion of infiltrating regulatory T-cells (Tregs) [121].
The expression of checkpoint molecules and the presence of immune cells in the meningioma microenvironment suggest that checkpoint blockade could be an effective therapeutic strategy. Two case studies have reported the use of PD-1 inhibitors in treating recurrent meningiomas, with one patient remaining disease-free for over two years and another for more than six months after undergoing nivolumab therapy. Both patients experienced reductions in tumor volume, cerebral edema, and symptom severity [117,118]. In contrast, Abele et al. reported the development of an atypical grade 2 meningioma in a patient receiving nivolumab for metastatic renal cell carcinoma. Currently, based on available evidence, two clinical trials are underway to assess the efficacy of anti-PD-1 antibodies in meningioma treatment (Table 3). Patient recruitment can be challenging, particularly for less common tumor types or in cases where patients have already undergone multiple treatments. Additionally, many patients may have operative or comorbidity considerations that render them ineligible for participation, thereby limiting the available population for studying new therapeutic approaches.
DownLoad:
CSV
| Immunotherapy | Trial identifier | Study title | Study start | Phase |
| Nivolumab | NCT03173950 | Immune checkpoint inhibitor nivolumab in people with recurrent select rare CNS cancers | 2017/7/13 | Phase 2 |
| Pembrolizumab | NCT04659811 | Stereotactic radiosurgery and immunotherapy (pembrolizumab) for the treatment of recurrent meningioma | 2021/3/25 | Phase 2 |
Pituitary adenomas are typically regarded as benign tumors; however, about 0.2% of cases can metastasize and are classified as pituitary carcinomas [122,123]. Refractory pituitary adenomas, which occupy an intermediate state between benign tumors and carcinomas, are characterized by a high Ki-67 proliferation index, aggressive growth, frequent recurrence, and notable resistance to chemotherapy [124–126]. The challenging nature of treating refractory pituitary adenomas and carcinomas stems from limited therapeutic options. In pursuit of a promising immunotherapy approach, ICIs have been experimentally employed for pituitary tumor treatment. In a patient with corticotroph carcinoma, experimental treatment with ipilimumab and nivolumab led to significant reductions in hormone levels and shrinkage of both the primary and metastatic lesions [127]. Nonetheless, a different patient diagnosed with corticotroph adenoma exhibited rapid progression of the disease following four cycles of pembrolizumab therapy [128]. At present, two clinical trials are registered to evaluate immunotherapeutic approaches for pituitary tumors. The first, a Phase 2 trial, investigates the efficacy of combining nivolumab and ipilimumab in individuals with aggressive pituitary tumors (NCT04042753). The second trial explores the same combination treatment for rare tumor types, including pituitary tumors (NCT02834013). Though patient recruitment for both trials has been completed, no results have been reported yet. Notably, there are currently no active clinical trials recruiting patients, and progress in related studies appears stagnant. This situation underscores the urgent need for additional preclinical and clinical investigations to explore the efficacy of immunotherapy in pituitary tumors.
This study conducts a bibliometric analysis to elucidate the current landscape of research concerning the immunotherapy of brain metastases, gliomas, meningiomas, and pituitary adenomas. Visual analysis showed a steady upward trend in brain metastasis and glioma immunotherapy research. In contrast, research into immunotherapy for meningiomas and pituitary adenomas is still at an early stage. The USA and China have made significant contributions in all four areas of research. Enhancing collaboration and communication among scientists, countries, and organizations is essential for advancing research in these areas and uncovering new opportunities for exploration. Currently, research on immunotherapy for brain tumors is mainly focused on exploring the synergistic effects of combining ICIs with conventional treatments. The investigation of the different types of immunotherapies, especially ICIs, and their clinical efficacy in brain tumors will remain a highly relevant and exciting area of research for the near future.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Donghu Yu: Writing – original draft, Methodology, Investigation, Data curation. Junneng Wang: Software, Formal analysis, Data curation. Lei Hu: Visualization, Validation, Methodology, Formal analysis, Data curation. Youxian Wu: Visualization, Software, Formal analysis, Data curation. Tianqing Wang: Validation, Data curation. Zhiyu Li: Visualization, Validation, Supervision. Zefen Wang: Software, Resources, Methodology, Formal analysis. Qihang Ding: Writing – original draft, Supervision, Software. Yao Sun: Writing – review & editing, Project administration, Investigation, Conceptualization. Zhiqiang Li: Project administration, Methodology, Investigation.
This research was supported by the National Natural Science Foundation of China (No. 82273328), and Hubei Province Key Research & Development Program (No. 2021BCA143).
Supplementary material associated with this article can be found, in the online version, at doi:
P. Sharma, B.A. Siddiqui, S. Anandhan, et al., Cancer Discov. 11 (2021) 838–857. doi: 10.1158/2159-8290.cd-20-1680
A.D. Waldman, J.M. Fritz, M.J. Lenardo, Nat. Rev. Immunol. 20 (2020) 651–668. doi: 10.1038/s41577-020-0306-5
C. Garbe, R. Dummer, T. Amaral, et al., Nat. Med. 29 (2023) 1310–1312. doi: 10.1038/s41591-023-02336-1
A.C. Huang, R. Zappasodi, Nat. Immunol. 23 (2022) 660–670. doi: 10.1038/s41590-022-01141-1
G. Casirati, A. Cosentino, A. Mucci, et al., Nature 621 (2023) 404–414. doi: 10.1038/s41586-023-06496-5
L. Tang, Z. Huang, H. Mei, Y. Hu, Signal. Transduct. Target. Ther. 8 (2023) 306. doi: 10.1038/s41392-023-01521-5
J.G. Lyon, N. Mokarram, T. Saxena, S.L. Carroll, R.V. Bellamkonda, Adv. Drug Deliv. Rev. 114 (2017) 19–32. doi: 10.1016/j.addr.2017.06.006
A. Sabbagh, K. Beccaria, X. Ling, et al., Clin. Cancer Res. 27 (2021) 4325–4337. doi: 10.1158/1078-0432.ccr-20-3760
F. Bai, Y. Deng, L. Li, et al., Exploration 4 (2024) 20230177. doi: 10.1002/EXP.20230177
A. Zhang, K. Miao, H. Sun, C.X. Deng, Int. J. Biol. Sci. 18 (2022) 3019–3033. doi: 10.7150/ijbs.72534
A. Ahmad, P. Khan, A.U. Rehman, S.K. Batra, M.W. Nasser, Mol. Cancer 22 (2023) 111. doi: 10.1186/s12943-023-01818-7
J.H. Suh, R. Kotecha, S.T. Chao, et al., Nat. Rev. Clin. Oncol. 17 (2020) 279–299. doi: 10.1038/s41571-019-0320-3
A.M. Di Giacomo, M. Valente, A. Cerase, et al., J. Exp. Clin. Cancer Res. 38 (2019) 419. doi: 10.1186/s13046-019-1426-2
P.K.K. Brastianos, A.E.E. Kim, A. Giobbie-Hurder, et al., Nat. Med. 29 (2023) 1728. doi: 10.1038/s41591-023-02392-7
E. Nieblas-Bedolla, N. Nayyar, M. Singh, R.J. Sullivan, P.K. Brastianos, Oncologist 26 (2021) 231–241. doi: 10.1002/onco.13575
K.J. Habashy, R. Mansour, C. Moussalem, R. Sawaya, M.J. Massaad, Br. J. Cancer 127 (2022) 976–987. doi: 10.1038/s41416-022-01864-w
D.N. Louis, A. Perry, P. Wesseling, et al., Neuro Oncol. 23 (2021) 1231–1251. doi: 10.1093/neuonc/noab106
T.F. Cloughesy, A.Y. Mochizuki, J.R. Orpilla, et al., Nat. Med. 25 (2019) 477. doi: 10.1038/s41591-018-0337-7
K.A. Schalper, M.E. Rodriguez-Ruiz, R. Diez-Valle, et al., Nat. Med. 25 (2019) 470. doi: 10.1038/s41591-018-0339-5
Q.T. Ostrom, M. Price, C. Neff, et al., Neuro Oncol. 24 (2022) v1–v95. doi: 10.1093/neuonc/noac202
J. Moliterno, W.P. Cope, E.D. Vartanian, et al., J. Neurosurg. 123 (2015) 23–30. doi: 10.3171/2014.10.JNS14502
M. Terabe, J. Wu, Neuro Oncol. 23 (2021) 1812–1813. doi: 10.1093/neuonc/noab168
G. Medici, L.K. Freudenmann, J. Velz, et al., Acta Neuropathol. 146 (2023) 173–190. doi: 10.1007/s00401-023-02605-w
T. Feola, F. Carbonara, M. Verrico, et al., Cancers 14 (2022) 4093. doi: 10.3390/cancers14174093
G. Raverot, M.D. Ilie, H. Lasolle, et al., Nat. Rev. Endocrinol. 17 (2021) 671–684. doi: 10.1038/s41574-021-00550-w
C. Dai, S. Liang, B. Sun, J. Kang, Front. Endocrinol. 11 (2020) 608422. doi: 10.3389/fendo.2020.608422
Y. Mei, W.L. Bi, N.F. Greenwald, et al., Oncotarget 7 (2016) 76565–76576. doi: 10.18632/oncotarget.12088
Y.D. Miao, W. Quan, X. Dong, et al., Cell. Death. Discov. 9 (2023) 129. doi: 10.1038/s41420-023-01421-1
S.E.H. Zyoud, S.W. Al-Jabi, R. Amer, et al., J. Transl. Med. 20 (2022) 83. doi: 10.1186/s12967-022-03293-y
Z. Shen, J. Hu, H. Wu, et al., J. Transl. Med. 20 (2022) 409. doi: 10.1186/s12967-022-03615-0
J. Jin, Y. Wan, Q. Shu, J. Liu, D. Lai, Front. Immunol. 14 (2023) 1158323. doi: 10.3389/fimmu.2023.1158323
M. Aria, C. Cuccurullo, J. Informetrics 11 (2017) 959–975. doi: 10.1016/j.joi.2017.08.007
N.J. van Eck, L. Waltman, Scientometrics 84 (2010) 523–538. doi: 10.1007/s11192-009-0146-3
S.B. Goldberg, S.N. Gettinger, A. Mahajan, et al., Lancet Oncol. 17 (2016) 976–983. doi: 10.1016/S1470-2045(16)30053-5
C.E. Brown, D. Alizadeh, R. Starr, et al., N. Engl. J. Med. 375 (2016) 2561–2569. doi: 10.1056/NEJMoa1610497
S.J. Han, G. Reis, G. Kohanbash, et al., J. Neuro Oncol. 130 (2016) 543–552. doi: 10.1007/s11060-016-2256-0
J.H. Sampson, M.D. Gunn, P.E. Fecci, D.M. Ashley, Nat. Rev. Cancer 20 (2020) 12–25. doi: 10.1038/s41568-019-0224-7
J.D. Bernstock, K.D. Kang, N.V. Klinger, et al., Oncogene 41 (2022) 2663–2671. doi: 10.1038/s41388-022-02312-y
C.E. Brown, S. Bucktrout, L.H. Butterfield, et al., J. Transl. Med. 20 (2022) 236. doi: 10.1186/s12967-022-03438-z
G.V. Long, V. Atkinson, S. Lo, et al., Lancet Oncol. 19 (2018) 672–681. doi: 10.1016/S1470-2045(18)30139-6
H.M. Kluger, V. Chiang, A. Mahajan, et al., J. Clin. Oncol. 37 (2019) 52. doi: 10.1200/jco.18.00204
H. Zhang, H. Yu, G. Zhao, et al., Front. Endocrinol. 14 (2023) 1273634. doi: 10.3389/fendo.2023.1273634
Y. Yuan, Y. Su, Y. Wu, et al., Front. Oncol. 13 (2023) 1229905. doi: 10.3389/fonc.2023.1229905
M. Lim, Y. Xia, C. Bettegowda, M. Weller, Nat. Rev. Clin. Oncol. 15 (2018) 422–442. doi: 10.1038/s41571-018-0003-5
D.A. Reardon, A.A. Brandes, A. Omuro, et al., JAMA Oncol. 6 (2020) 1003–1010. doi: 10.1001/jamaoncol.2020.1024
D.M. O'Rourke, M.P. Nasrallah, A. Desai, et al., Sci. Transl. Med. 9 (2017) eaaa0984. doi: 10.1126/scitranslmed.aaa0984
M. Ding, A. Zhu, Y. Zhang, et al., Nano Today 57 (2024) 102398. doi: 10.1016/j.nantod.2024.102398
H. Chen, T. Li, Z. Liu, et al., Nat. Commun. 14 (2023) 941. doi: 10.1038/s41467-022-35709-0
T. Wang, H. Zhang, W. Qiu, et al., Bioact. Mater. 16 (2022) 418–432.
D. Yu, M. Liu, Q. Ding, et al., Biomaterials 316 (2025) 123021. doi: 10.1016/j.biomaterials.2024.123021
F. Ghiringhelli, C. Rebe, Immunol. Rev. 321 (2024) 335–349. doi: 10.1111/imr.13263
L. Tu, C. Li, Q. Ding, et al., J. Am. Chem. Soc. 146 (2024) 8991–9003. doi: 10.1021/jacs.3c13224
W.L. Bi, L. Nayak, D.M. Meredith, et al., Neuro Oncol. 24 (2022) 101–113. doi: 10.1093/neuonc/noab118
M.D. Ilie, C. Villa, T. Cuny, et al., Eur. J. Endocrinol. 187 (2022) 685–696. doi: 10.1530/eje-22-0647
Y. Zhang, Z. Zhang, Cell. Mol. Immunol. 17 (2020) 807–821. doi: 10.1038/s41423-020-0488-6
L. Kraehenbuehl, C.H. Weng, S. Eghbali, J.D. Wolchok, T. Merghoub, Nat. Rev. Clin. Oncol. 19 (2022) 37–50. doi: 10.1038/s41571-021-00552-7
A. Peri, N. Salomon, Y. Wolf, et al., Nat. Cancer 4 (2023) 937–954. doi: 10.1038/s43018-023-00588-x
L.K. Donovan, M.D. Taylor, Cell Res. 32 (2022) 505–506. doi: 10.1038/s41422-022-00649-3
K. Yang, A. Halima, T.A. Chan, Nat. Rev. Clin. Oncol. 20 (2023) 604–623. doi: 10.1038/s41571-023-00789-4
M. Ramos-Casals, J.R. Brahmer, M.K. Callahan, et al., Nat. Rev. Dis. Primers 6 (2020) 38. doi: 10.1038/s41572-020-0160-6
Q. Sun, Z. Hong, C. Zhang, et al., Signal Transduc. Target. Ther. 8 (2023) 320. doi: 10.1038/s41392-023-01522-4
D.J. Baker, Z. Arany, J.A. Baur, J.A. Epstein, C.H. June, Nature 619 (2023) 707–715. doi: 10.1038/s41586-023-06243-w
C.H. June, R.S. O'Connor, O.U. Kawalekar, S. Ghassemi, M.C. Milone, Science 359 (2018) 1361–1365. doi: 10.1126/science.aar6711
K.M. Cappell, J.N. Kochenderfer, Nat. Rev. Clin. Oncol. 20 (2023) 359–371. doi: 10.1038/s41571-023-00754-1
Y. Xie, X. Li, J. Wu, et al., Chin. Chem. Lett. 34 (2023) 108202. doi: 10.1016/j.cclet.2023.108202
S.A. Rosenberg, J.C. Yang, N.P. Restifo, Nat. Med. 10 (2004) 909–915. doi: 10.1038/nm1100
M.J. Lin, J. Svensson-Arvelund, G.S. Lubitz, et al., Nat. Cancer 3 (2022) 911–926. doi: 10.1038/s43018-022-00418-6
J. Adamik, L.H. Butterfield, Sci. Transl. Med. 14 (2022) eabo4632. doi: 10.1126/scitranslmed.abo4632
M. Tagliamonte, B. Cavalluzzo, A. Mauriello, et al., Mol. Cancer 22 (2023) 75. doi: 10.1186/s12943-023-01776-0
D. Lin, Y. Shen, T. Liang, Signal Transduc. Target. Ther. 8 (2023) 156. doi: 10.1038/s41392-023-01407-6
S.Z. Shalhout, D.M. Miller, K.S. Emerick, H.L. Kaufman, Nat. Rev. Clin. Oncol. 20 (2023) 160–177. doi: 10.1038/s41571-022-00719-w
A.K. Park, Y. Fong, S.I. Kim, et al., Sci. Transl. Med. 12 (2020) eaaz1863. doi: 10.1126/scitranslmed.aaz1863
C. Hajal, Y. Shin, L. Li, et al., Sci. Adv. 7 (2021) eabg8139. doi: 10.1126/sciadv.abg8139
J.D. Hebert, J.W. Neal, M.M. Winslow, Nat. Rev. Cancer 23 (2023) 391–407. doi: 10.1038/s41568-023-00568-4
T.K. Owonikoko, J. Arbiser, A. Zelnak, et al., Nat. Rev. Clin. Oncol. 11 (2014) 203–222. doi: 10.1038/nrclinonc.2014.25
M.A. Davies, P. Liu, S. McIntyre, et al., Cancer 117 (2011) 1687–1696. doi: 10.1002/cncr.25634
J.T. Moyers, E.G. Chong, J. Peng, et al., Cancer Med. 10 (2021) 1201–1211. doi: 10.1002/cam4.3716
A. Lauko, R. Kotecha, A. Barnett, et al., Sci. Rep. 11 (2021) 18174. doi: 10.1038/s41598-021-97566-z
S. Kang, H. Jeong, J.E. Park, et al., Ann. Oncol. 33 (2022) S1081–S1082.
A. Le, H. Mohammadi, T. Mohammed, et al., J. Neuro Oncol. 158 (2022) 481–488. doi: 10.1007/s11060-022-04038-z
V. Borzillo, R. Di Franco, D. Giannarelli, et al., Cancers 13 (2021) 1857. doi: 10.3390/cancers13081857
T. Amaral, F. Kiecker, S. Schaefer, et al., J. Immunother. Cancer 8 (2020) e000333. doi: 10.1136/jitc-2019-000333
I. Hadi, O. Roengvoraphoj, R. Bodensohn, et al., Radiat. Oncol. 15 (2020) 37. doi: 10.1186/s13014-020-1485-8
J. Liermann, J.K. Winkler, M. Syed, et al., Front. Oncol. 10 (2020) 592796. doi: 10.3389/fonc.2020.592796
T.L. Enright, J.S. Witt, A.R. Burr, et al., Clin. Lung Cancer 22 (2021) 110–119. doi: 10.1016/j.cllc.2020.10.014
A. Cho, H. Untersteiner, D. Hirschmann, et al., Cancers 12 (2020) 3668. doi: 10.3390/cancers12123668
S. Scoccianti, E. Olmetto, V. Pinzi, et al., Neuro-Oncol. 23 (2021) 1750–1764. doi: 10.1093/neuonc/noab129
M. Abdulhaleem, H. Johnston, R. D'Agostino Jr., et al., J. Neuro-Oncol. 157 (2022) 101–107. doi: 10.1007/s11060-022-03951-7
T. Amaral, I. Tampouri, T. Eigentler, et al., Immunotherapy 11 (2019) 297–309. doi: 10.2217/imt-2018-0149
P.D. Banks, A. Lasocki, P.K.H. Lau, et al., Health. Sci. Rep. 2 (2019) e115. doi: 10.1002/hsr2.115
Z. Ye, X. Ai, L. Zhao, et al., Oncogene 40 (2021) 6059–6070. doi: 10.1038/s41388-021-02010-1
J.R.D. Pearson, T. Regad, Signal Transduct. Target. Ther. 2 (2017) 17040. doi: 10.1038/sigtrans.2017.40
J.P. Lynes, A.K. Nwankwo, H.P. Sur, et al., J. Immunother. Cancer 8 (2020) e000348. doi: 10.1136/jitc-2019-000348
D. Yu, Q. Zhong, Y. Xiao, et al., NPJ Precis. Oncol. 8 (2024) 140. doi: 10.1038/s41698-024-00632-8
A. Rusak, B. Wiatrak, K. Krawczynska, et al., Transl. Oncol. 51 (2025) 102187. doi: 10.1016/j.tranon.2024.102187
M. Vanneman, G. Dranoff, Nat. Rev. Cancer 12 (2012) 237–251. doi: 10.1038/nrc3237
C.N. Baxevanis, A.D. Gritzapis, I.F. Voutsas, et al., Cancers 14 (2022) 2674. doi: 10.3390/cancers14112674
Z. Zhang, X. Liu, D. Chen, J. Yu, Signal Transduct. Target. Ther. 7 (2022) 258. doi: 10.1038/s41392-022-01102-y
D.S. Vinay, E.P. Ryan, G. Pawelec, et al., Semin. Cancer Biol. 35 (2015) S185–S198. doi: 10.1016/j.semcancer.2015.03.004
A.S. Luksik, E. Yazigi, P. Shah, C.M. Jackson, Cancers 15 (2023) 1414. doi: 10.3390/cancers15051414
S.I. Choi, J. Yin, Front. Immunol. 13 (2022) 1008751. doi: 10.3389/fimmu.2022.1008751
G. Dagar, A. Gupta, T. Masoodi, et al., J. Transl. Med. 21 (2023) 449. doi: 10.1186/s12967-023-04292-3
D.B. Keskin, A.J. Anandappa, J. Sun, et al., Nature 565 (2019) 234–239. doi: 10.1038/s41586-018-0792-9
M. Weller, N. Butowski, D.D. Tran, et al., Lancet Oncol. 18 (2017) 1373–1385. doi: 10.1016/S1470-2045(17)30517-X
B. Segura-Collar, S. Hiller-Vallina, O. de Dios, et al., Acta Neuropathol. Commun. 11 (2023) 79. doi: 10.1186/s40478-023-01569-y
R.T. Merrell, P.Y. Wen, D.A. Forst, et al., J. Clin. Oncol. 42 (2024) TPS2100. doi: 10.1200/jco.2024.42.16_suppl.tps2100
T. Todo, H. Ito, Y. Ino, et al., Nat. Med. 28 (2022) 1630–1639. doi: 10.1038/s41591-022-01897-x
P. Liu, Y. Wang, Y. Wang, et al., Gene Ther. 29 (2022) 115–126. doi: 10.1038/s41434-020-00207-9
Q. Zhang, F. Liu, Cell Death Dis. 11 (2020) 485. doi: 10.1038/s41419-020-2696-5
N. Aldrak, S. Alsaab, A. Algethami, et al., Cells 10 (2021) 1541. doi: 10.3390/cells10061541
N. Ji, D. Weng, C. Liu, et al., Oncotarget 7 (2016) 4369–4378. doi: 10.18632/oncotarget.6737
A. Bianconi, G. Palmieri, G. Aruta, et al., Biomedicines 11 (2023) 1520. doi: 10.3390/biomedicines11061520
Q.T. Ostrom, G. Cioffi, H. Gittleman, et al., Neuro Oncol. 21 (2019) V1–V100. doi: 10.1093/neuonc/noz150
L. Rogers, I. Barani, M. Chamberlain, et al., J. Neurosurg. 122 (2015) 4–23. doi: 10.3171/2014.7.JNS131644
T. Garzon-Muvdi, D.D. Bailey, M.N. Pernik, E. Pan, Front. Neurol. 11 (2020) 945. doi: 10.3389/fneur.2020.00945
D.T. Proctor, Z. Patel, S. Lama, et al., Oncoimmunology 8 (2018) e1512943.
E. Gelerstein, A. Berger, T. Jonas-Kimchi, et al., J. Clin. Neurosci. 37 (2017) 51–53. doi: 10.1016/j.jocn.2016.11.011
I.E. Dunn, Z. Du, M. Touat, et al., JCO Precis. Oncology 2 (2018) 1–12. doi: 10.1200/po.18.00190
P.H. Domingues, C. Teodosio, J. Ortiz, et al., Am. J. Pathol. 181 (2012) 1749–1761. doi: 10.1016/j.ajpath.2012.07.033
L. Fang, D.E. Lowther, M.L. Meizlish, et al., Neuro Oncol. 15 (2013) 1479–1490. doi: 10.1093/neuonc/not110
Y.D. Li, D. Veliceasa, J. Lamano, et al., Cancer Immunol. Immunother. 68 (2019) 999–1009. doi: 10.1007/s00262-019-02342-8
M.E. Molitch, JAMA 317 (2017) 516–524. doi: 10.1001/jama.2016.19699
T.M. Hansen, S. Batra, M. Lim, et al., Neurosurg. Rev. 37 (2014) 279–285. doi: 10.1007/s10143-014-0525-y
L. Kasuki, G. Raverot, Rev. Endocrine Metab. Disord. 21 (2020) 203–208. doi: 10.1007/s11154-019-09531-x
G. Raverot, P. Burman, A. McCormack, et al., Eur. J. Endocrinol. 178 (2018) G1–G24. doi: 10.1530/EJE-17-0796
M.B.S. Lopes, Acta Neuropathol. 134 (2017) 521–535. doi: 10.1007/s00401-017-1769-8
A.L. Lin, P. Jonsson, V. Tabar, et al., J. Clin. Endocrinol. Metab. 103 (2018) 3925–3930. doi: 10.1210/jc.2018-01347
M. Caccese, M. Barbot, F. Ceccato, et al., Anticancer Drugs 31 (2020) 199–203. doi: 10.1097/cad.0000000000000856

Figure 1 Annual publication trends in immunotherapy for brain metastasis, glioma, meningioma, and pituitary adenoma.

Figure 2 Top 10 authors with the highest number of publications in immunotherapy for (A) brain metastasis, (B) glioma, (C) meningioma, and (D) pituitary adenoma.

Figure 3 The keyword co-occurrence networks for publications on immunotherapy including (A) brain metastasis, (B) glioma, (C) meningioma, and (D) pituitary adenoma. Lines connecting nodes indicate the co-occurrence of keywords, with each node representing an individual keyword. Node size reflects the frequency of occurrences.

Figure 4 Mechanisms of current immunotherapies employed in brain tumors. ICIs, including PD-1, PD-L1, and CTLA-4 inhibitors, aim to counter T cell exhaustion by blocking immune checkpoints. This restoration of T cell function and reactivation of antitumor activity are key goals of ICIs. CAR therapies involve the genetic modification of a patient's T cells to express CARs specific to neoantigens. These engineered T cells are then expanded in culture and subsequently administered to the patient. Tumor vaccines work by stimulating anti-tumor immune responses through the targeting of antigen-presenting cells (APCs) with tumor antigens. OVs have the ability to directly lyse glioma cells, resulting in the release of tumor cell lysates that can trigger anti-tumor immune responses (created with BioRender.com).
Table 1. Immunotherapy clinical trials currently recruiting patients for the treatment of brain metastasis.
| Immunotherapy | Trial identifier | Study title | Study start | Phase |
| Pembrolizumab or combination of ipilimumab and nivolumab | NCT03563729 | Melanoma metastasized to the brain and steroids | 2018/6/6 | Phase 2 |
| CAR T cell | NCT03696030 | HER2-CAR T cells in treating patients with recurrent brain or leptomeningeal metastases | 2018/8/31 | Phase 1 |
| Combination of dendritic cell vaccines against Her2/Her3 and pembrolizumab | NCT04348747 | Dendritic cell vaccines against Her2/Her3 and pembrolizumab for the treatment of brain metastasis from triple negative breast cancer or HER2+ breast cancer | 2022/12/19 | Phase 2 |
 下载: 导出CSV
下载: 导出CSV
Table 2. Immunotherapy clinical trials currently recruiting patients for the treatment of glioma.
| Immunotherapy | Trial identifier | Study title | Study start | Phase |
| Pembrolizumab | NCT04977375 | Trial of anti-PD-1 immunotherapy and stereotactic radiation in patients with recurrent glioblastoma | 2021/12/9 | Phase 1/2 |
| Pembrolizumab | NCT05235737 | The assessment of immune response in newly diagnosed glioblastoma patients treated with pembrolizumab | 2022/3/1 | Phase 4 |
| Daratumumab | NCT04922723 | Radiation/temozolomide and immunotherapy with daratumumab to improve antitumor efficacy in glioblastoma | 2022/10/3 | Phase 1/2 |
| Combination of AB154 and AB122 | NCT04656535 | AB154 combined with AB122 for recurrent glioblastoma | 2021/4/21 | Phase 1 |
| Combination of D2C7-IT and 2141-V11 | NCT05734560 | D2C7-IT and 2141-V11 in newly diagnosed GBM patients | 2023/9/6 | Phase 1/2 |
| CARv3-TEAM-E T cell | NCT05660369 | CARv3-TEAM-E T cells in glioblastoma | 2023/3/22 | Phase 1 |
| C7R-GD2.CAR T cell | NCT04099797 | C7R-GD2.CAR T cells for patients with GD2-expressing brain tumors | 2020/2/3 | Phase 1 |
| B7H3-specific CAR T cell | NCT04185038 | Study of B7-H3-Specific CAR T cell locoregional immunotherapy for diffuse intrinsic pontine glioma/diffuse midline glioma and recurrent or refractory pediatric central nervous system tumors | 2019/12/11 | Phase 1 |
| B7-H3, EGFR806, HER2, And IL13-Zetakine CAR T cell | NCT05768880 | Study of B7-H3, EGFR806, HER2, and IL13-zetakine (Quad) CAR T cell locoregional immunotherapy for pediatric diffuse intrinsic pontine glioma, diffuse midline glioma, and recurrent or refractory central nervous system tumors | 2023/5/5 | Phase 1 |
| CD70 CAR T cell | NCT05353530 | Phase I study of IL-8 receptor-modified CD70 CAR T cell therapy in CD70+ and MGMT-unmethylated adult glioblastoma (IMPACT) | 2023/7/25 | Phase 1 |
| TVI-Brain-1 | NCT05685004 | Study of neoantigen-specific adoptive T cell therapy for newly diagnosed MGMT negative GBM | 2023/9/15 | Phase 1/2 |
| H3K27M peptide vaccine | NCT04808245 | A multicenter phase Ⅰ peptide vaccine trial for the treatment of H3-mutated gliomas | 2023/2/15 | Phase 1 |
| TTRNA-xALT | NCT04837547 | PEACH TRIAL-precision medicine and adoptive cellular therapy | 2021/9/20 | Phase 1 |
| Dendritic cell vaccine | NCT04801147 | Immunotherapy with autologous tumor lysate-loaded dendritic cells in patients with newly diagnosed GBM | 2010/6/1 | Phase 1/2 |
| DOTAP liposome vaccine | NCT04573140 | A study of RNA-lipid particle (RNA-LP) vaccines for newly diagnosed pediatric high-grade gliomas (pHGG) and adult glioblastoma (GBM) | 2021/10/26 | Phase 1 |
| VBI-1901 | NCT03382977 | Study to evaluate safety, tolerability, and optimal dose of candidate GBM vaccine VBI-1901 in recurrent GBM subjects | 2017/12/6 | Phase 1/2 |
| rQNestin34.5v.2 | NCT03152318 | A study of the treatment of recurrent malignant glioma with rQNestin34.5v.2 | 2017/7/18 | Phase 1 |
下载: 导出CSV
Table 3. Immunotherapy clinical trials currently recruiting patients for the treatment of meningioma.
| Immunotherapy | Trial identifier | Study title | Study start | Phase |
| Nivolumab | NCT03173950 | Immune checkpoint inhibitor nivolumab in people with recurrent select rare CNS cancers | 2017/7/13 | Phase 2 |
| Pembrolizumab | NCT04659811 | Stereotactic radiosurgery and immunotherapy (pembrolizumab) for the treatment of recurrent meningioma | 2021/3/25 | Phase 2 |
下载: 导出CSV

 扫一扫看文章
扫一扫看文章

扫一扫关注我们