Figure 1.
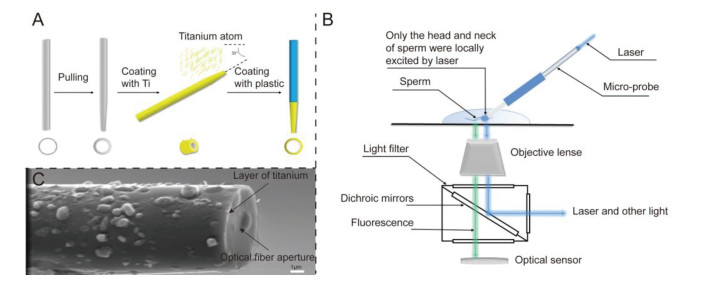
(A) The preparation of the capillary with the Ti ring at the microtip. (B) Schematics of the platform for fluorescence detection. (C) FE-SEM image of the optical micro-probe. Scale bar is 1 µm.
A new method for evaluating the quality of single sperm by detecting reactive oxygen species
Hao Hu , Bei Yan , Wei Zhang , Wenbo Yan , Liquan Liu , Xiaofeng Tang , Kejun Dong , Longjie Li , Xianjin Xiao , Chengliang Xiong

Infertility has been defined as having not taken any contraceptive measures for more than 1 year, a normal sex life, and no successful pregnancy [1]. In recent years, the incidence of infertility has increased annually. According to the World Health Organization (WHO) statistics, infertility has affected 8%−12% of couples in the reproductive age group, with 50% of these cases being related to male factors [2, 3]. The occurrence and development of male infertility is related to a variety of factors, including changes in lifestyle [4, 5], genetic causes [6, 7], and body damage caused by reactive oxygen species ROS [8]. Sperm damage caused by ROS is one of the main causes of male infertility. ROS refers to a class of oxygen-containing substances that have a high oxidizing capacity in the body or natural environment, including superoxide anions (O2•−), hydrogen peroxide (H2O2), hydroxyl (•OH), and peroxyl (•ROO) [9]. The mechanism of excessive ROS damages to sperm includes two aspects: (1) ROS directly destroys the sperm DNA in the cell nucleus and mitochondria [10], and (2) ROS leads to the peroxidation of sperm cell membrane lipids, triggering axonemal injury and causing ATP deficiency in the sperm, which ultimately affects sperm motility [11, 12]. In conclusion, excessive ROS in sperm has an important impact on male infertility; therefore, the level of ROS in sperm is an important indicator for the diagnosis and treatment of male infertility [13, 14].
At present, the main methods for detecting ROS in sperm are a chemiluminescence (CL) assay and flow cytometry (FCM) [15, 16]. The CL assay uses luminol as a luminescent agent; luminol is oxidized by ROS to emit a light signal, which is then detected by a CL meter to reflect the level of ROS in the sperm. However, the ROS detected by this method is the sum of sperm and seminal plasma ROS levels. The seminal plasma ROS level is greatly affected by the surrounding environment; therefore, this method cannot accurately reflect the sperm ROS level. Importantly, the level of ROS in sperm, and not that in semen, is the indicator that best reflects the quality of sperm and male fertility.
To overcome the difficulty that the CL assay cannot directly detect sperm ROS, researchers employed FCM to detect sperm ROS. The principle of FCM detection of ROS is to excite the fluorescent probe (such as 2′, 7′-dichlorodi-hydrofluorescein diacetate, DCFH-DA) and then collect the signal. The probe alone does not emit a fluorescent signal and can freely pass through the cell membrane. However, after the probe enters the sperm and is oxidized by ROS, it can no longer penetrate the sperm. The probe in the sperm is then excited by the laser, and emits a fluorescent signal. The detection method can produce a specific response to ROS in the sperm cells. However, the flow cytometer divides the tested sample into individual droplets that pass through the detection area. Although each droplet contains one cell, the detected signal is the fluorescence intensity of the entire droplet, which cannot accurately detect the fluorescence intensity of the sperm. In addition, the excitation light of the flow cytometer is focused on a specific plane. For different sperm, even if they have the same ROS level (concentration of fluorescent substance in the cell), they will show different detection results due to the difference in the focal plane. Therefore, FCM cannot accurately measure the intracellular fluorescence signal of the sperm.
In summary, evaluation of the ROS level has important guiding significance for evaluating sperm quality and in the prognostic assessment, educational diagnosis, and antioxidant treatment of male infertility. However, a method for accurately quantifying a single spermatic ROS level is currently lacking.
In this study, we constructed a single sperm ROS detection method (SSRDM). The method is divided into two steps: First, we used 5-(and-6)-chloromethyl-2′, 7′-dichlorodihydrofluorescein diacetate (CM-H2DCFDA) to fluorescently stain ROS in the sperm. This compound is typically loaded into sperm in the form of a membrane-permeant diacetate (DA) ester. Then, intracellularly, it is converted into non-fluorescent CM-H2DCF by esterase action. After that, cellular oxidant stimulates the formation of CM-DCF from CM-H2DCF through a peroxide-catalyzed reaction, which involves two main steps: (1) conversion of CM-H2DCF into CM-DCFH•/CM-DCF•− stimulated by CO3•−, NO2• and/or peroxidase-like catalysts involving conversion of GS• into GSH, (2) formation of CM-DCF stimulated by generation of O2•− from O2. And the chloromethyl on fluorescent CM-DCF prompts it more negatively charged, making it difficult to penetrate the sperm membrane. The lack of specificity of CM-DCF formation makes it difficult to identify the nature of the oxidants detected by the probe. Therefore, the formation of CM-DCF in cellular systems can best be considered as a marker of cellular oxidant levels rather than as a direct reporter of a specific ROS species. After removing the extracellular free staining solution, CM-H2DCFDA could more specifically indicate the level of ROS in sperm cells. Second, we measured the fluorescent signal in a single sperm and introduced a unique optical micro-probe that is fabricated via a focused ion beam (FIB) process. The micro-probe is approximately 8 cm in length composed of three layers from the inside to the outside: an optical fiber layer, a titanium metal layer with a thickness of about 100 nm, and a 1 µm thick plastic wrap layer (Fig. 1A). This design allows the laser light to be irradiated from the probe to the cell through the optical fiber without damage. We would like to point out that the fundamental advantages of using micro-fiber to detect ROS are direct measurement and eliminated background signal. The claimed advantage of direct measurement is with respect to the clinically prevalent flow-cytometry method which only reports the percentage of sperm cells higher than cut-off. "The percentage of sperm cells" is actually a cell-level parameter, not a direct quantitative description of the ROS. Using an indirect cell-level parameter to describe the amount of molecule-level ROS is intrinsically deviated. As for the eliminated background signal, the size of the micro-fiber is around 6 µm, and therefore the diameter of the spherical exciting light emitted by the micro-fiber is also around 6 µm. Such small volume of spherical exciting light can only cover the head and neck of one sperm (which is also around 6 µm) and excite the fluorescent dyes within the pointed sperm head. As a result, the un-pointed sperms, interfering cells and surrounding buffer are not excited and will not produce any background signals [17]. Compared with conventional fluorescence microscopy which excites a thick layer of the sample, the background signal and the measurement deviations of our method are much lower. As shown in Fig. 1B, we built a fluorescence detection platform based on a laser micro-probe. We placed the micro-probe on the sperm head, which emits the corresponding excitation light according to the dye excitation wavelength and is confined to the sperm head and neck area; the scattered light is then received to obtain the fluorescence value A (Fig. S1 in Supporting information). This localized excitation method allows different sperm to receive the same excitation light intensity without being affected by the focal plane. The probe was then moved to excite the area around the sperm head, and the measured fluorescence was used as the background value B. The difference between A and B reflects the intracellular fluorescence intensity of the tested sperm. In summary, this method can accurately determine ROS level in a single sperm.
We first characterized the micro-probe. The field emission-scanning electron microscope (FE-SEM) image (Fig. 1C) of a typical optical micro-probe clearly revealed an optical fiber aperture surrounded by a ring of titanium. The aperture effectively confined the excitation light in the evanescent field with an extremely low penetration depth, leading to highly localized excitation. Furthermore, the reduced excitation intensity from the aperture could also minimize dye bleaching [18].
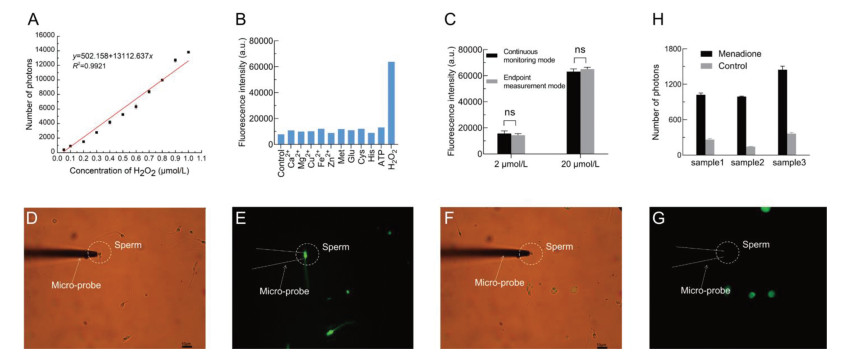
Further, we discussed the sensitivity, specificity and stability of CM-H2DCFDA in buffer. CM-H2DCFDA can be oxidized by the various ROS. Therefore, we cannot prepare standard solutions to produce a standard curve that can calculate the levels of mixed oxides. However, we can use standard solutions of H2O2 to create a standard curve of the number of photons over the concentration of H2O2. Subsequently, the number of photons produced by a certain sperm could be translated to a calculated concentration of H2O2, i.e., we could use the concentration of H2O2 as an equivalent parameter to quantitatively describe the amount of ROS in the sperm. In the concentration range of 0.05–1 µmol/L, the number of photons (after subtracting the background value) demonstrated a good linear regression relationship with H2O2 concentration (R2 = 0.9921) (Fig. 2A). The detection limit was calculated to be 0.01 µmol/L based on 3 σ/S, where σ is the standard deviation of a blank measurement and S is the slope of fluorescence intensity versus H2O2 concentration. The equation of the standard is NPs = −502.158 + 13, 112.637C, where NPs and C represent number of photons and the concentration of H2O2, respectively. Finally, we can calculate the amount of ROS of any sperm simply by plugging the number of photons into the above equation (The calculated result is the equivalent concentration of H2O2, not the real concentrations of mixed oxides). For specificity, we tested CM-H2DCFDA with 10 different ions and biomolecules. As shown in Fig. 2B, only H2O2 could trigger an obvious fluorescence increase. The other tested species showed a negligible effect relative to H2O2. For stability, we treated CM-H2DCFDA with 2 µmol/L and 20 µmol/L of H2O2 for 30 min. The fluorescent signals were recorded in two modes: the first mode was continuously monitoring the fluorescence intensity from the beginning to the endpoint (30 min), and the latter mode was incubating the reaction system (CM-H2DCFDA with 2 µmol/L and 20 µmol/L of H2O2) in dark for 30 min and only measuring the fluorescence intensity at the endpoint. Overall, CM-H2DCFDA in the first mode was exposed with exciting light for many times whereas it was exposed only once in the latter mode, so we could evaluate the photostability of our probe by comparing the endpoint fluorescent signals in such two modes. As presented in Fig. 2C, the end-point fluorescence intensity in two modes were very close (the difference was not significant), demonstrating the photostability of our probe.
Then 72 of 102 semen samples were performing standard semen analysis and the specific studied semen parameters for the samples were summarized in Table S1 (Supporting information). Based on the WHO guideline (2010), asthenozoospermia was defined as progressive motility < 32% in a semen sample [19]. According to the standard, we divided the 72 semen samples from infertility clinic and sperm bank into asthenozoospermia and non-asthenozoospermia groups. The average of the different semen parameters was calculated (Table 1). Overall, the non-asthenozoospermia group had significantly higher sperm progressive motility (P < 0.001) than the asthenozoospermia group. Sperm concentration (P = 0.284) and count (P = 0.269) were similar in both groups.
 DownLoad:
CSV
DownLoad:
CSV

|
To explore the effect of CM-H2DCFDA on the staining of ROS in sperm, we took the sperm suspension after incubation and observed it under a fluorescence microscope. As shown in Fig. S2 (Supporting information), the head and neck had a high ROS level compared to the background or other parts of the sperm, resulting in the emission of a very bright green fluorescence. This indicates that CM-H2DCFDA can be oxidized by ROS in sperm, and this is most obvious in the head and neck, which is consistent with the results of previous studies.
Next, we used SSRDM to detect sperm ROS in a sperm suspension. Here we are using photon-counting system, the measured value is the number of photons. Sperm with a higher fluorescence value (Figs. 2D and E, number of photons = 1796) appear as a bright spot under the fluorescence microscope, while sperm with a lower fluorescence value (Figs. 2F and G, number of photons = 26) had no bright spots. Moreover, the progressive motility < 32% in the sample showed in Figs. 2D and E. While, the sperm in Figs. 2F and G was non-asthenozoospermia. The capacity of CM-H2DCFDA and the micro-fiber probe was further studied using menadione as an ROS stimulant for monitoring the expression levels of upregulated ROS in sperm (Fig. 2H and Fig. S3 in Supporting information). The result above indicates that we have successfully established a micro-probe-based method for detecting intracellular ROS in sperm.
Then, to further explore the feasibility of this method in clinical applications, we tested the ROS in the sperm of 72 semen samples. The specific results are shown in Table S1. The average fluorescence value of the non-asthenozoospermia group was 400.75, while that of the asthenozoospermia group was 597.38 (Table 1 and Fig. S4 in Supporting information). The Mann-Whitney U test showed a significant between-group difference in the average fluorescence value (P = 0.002) (Table 1 and Fig. S4). Therefore, SSRDM can clearly distinguish the ROS levels of asthenozoospermia sperm and non-asthenozoospermia sperm, thereby providing a reliable basis for the determination of sperm quality.
Besides, the intracellular ROS of the 72 samples were also detected by FCM. Gate for sperm was set according to dot plot chart displaying characteristics of forward scatter, which is roughly proportional to the diameter of the cell, and side scatter, which is proportional to cellular granularity (Fig. S5 in Supporting information). The specific results are presented in Table S1. However, we notice that the proportion of luminous sperm in the asthenozoospermia group detected by FCM was approximately 30%, while the proportion in the non-asthenozoospermia group was approximately 23% (Table 1 and Fig. S4). The results of FCM were non-normally distributed, and the Mann-Whitney U test gave a P value of 0.152 (Table 1 and Fig. S4). Based on the above results, FCM cannot distinguish asthenospermic sperm from non-asthenospermic sperm in terms of ROS levels.
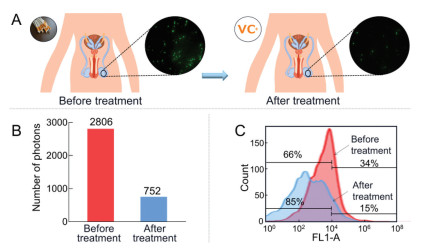
The above results indicate that SSRDM can be used to detect the level of ROS in sperm, thereby providing evidence for the assessment of sperm quality and the diagnosis of male infertility. In fact, this method can also evaluate the effect of andrology antioxidant therapy. One of the patients in the group likes smoking. Moreover, standard semen analysis showed that progressive motility of his sperm was weak; thus, we further detected ROS level in sperm. It was observed under the microscope that there were many bright sperm in the visual field (Fig. 3A). SSRDM results showed that fluorescence value of his sperm reached 2806 (Fig. 3B), while FCM indicated the proportion of luminescent sperm in the semen reached 34% (Fig. 3C). After taking the antioxidant drugs of astaxanthin and vitamin C for one and a half months, we detected ROS level in his sperm again. Microscopic examination, SSRDM and FCM all showed that the level of ROS in sperm was significantly decreased. Therefore, SSRDM is also a reliable tool for evaluating the prognosis of antioxidant therapy.
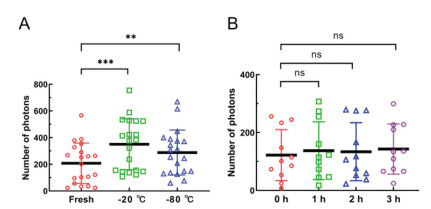
ROS level in sperm is easily affected by the external environment, especially related to factors such as the storage temperature and time after liquefaction. Therefore, we investigated the temperature variability (Table S2 in Supporting information) and temporal variability (Table S3 in Supporting information) of SSRDM to optimize the detection conditions. Firstly, the results of paired t-test indicated that, compared with fresh samples, the ROS levels in sperm that were frozen at −20 ℃ and −80 ℃ showed significant differences (P < 0.05) (Fig. 4A). Consistent with the findings of previous studies, ice crystals produced at low temperature severely impact the formation of sperm ROS. Subsequently, we also explored the effect of time that liquefied semen specimens placed in a 37 ℃ water bath, on the results of SSRDM. The results of paired t-test showed that there was no statistically significant difference between the ROS of the sperm placed for 1 h (P = 0.889), 2 h (P = 0.654), 3 h (P = 0.709) and 0 h (Fig. 4B). The above conclusions manifested that to ensure the stability and accuracy of SSRDM, the specimens can be measured within 3 h and are not suitable for storage at low temperature.
There is overwhelming evidence that ROS play a significant role in male infertility [20]. However, current clinical methods cannot accurately measure the level of ROS in sperm cells, which makes it difficult to accurately diagnose the cause of male infertility. In this study, we developed a new method for detecting ROS in sperm. This method uses a micron-level fiber optic probe to specifically excite oxidized CM-H2DCFDA in the head and neck of the sperm to achieve the quantitative detection of ROS in the sperm. In addition, in terms of ROS levels, compared with FCM, SSRDM has a stronger ability to distinguish between asthenozoospermia sperm and non-asthenozoospermia sperm, which provides more reliable evidence for the assessment of sperm quality and the diagnosis of male infertility. We further prove that this method can also be used to evaluate the effect of antioxidant treatment. Moreover, temperature variability and temporal variability of SSRDM are also investigated to optimize the detection conditions.
Compared with other clinical methods for detecting ROS in sperm, the SSRDM has the main advantage of being able to remove non-specific background values relatively accurately, thereby measuring the level of ROS in sperm. Because the traditional CL assay cannot remove ROS detected in the seminal plasma, such as the ROS produced by white blood cells, the measured ROS level cannot truly reflect that in the sperm. The flow cytometer uses the fluorescence of the unstained sperm as the background signal. However, ROS fluorescent dye can still pass out the sperm cell membrane after being oxidized, resulting in a certain difference between the background signal of the sperm-containing droplet and the set background signal, resulting in an inaccurate detection of ROS.
Although the method we developed has great advantages, it also has some shortcomings. First, the detection throughput of this method was not high. Specifically, our method can only detect approximately 60 sperms in 30 min. The main reason for this problem is the low degree of automation of the fluorescence detection platform; at present, our platform can only use a robotic arm to hold a light probe, and the human eye needs to assist the micro-probe to point to the sperm. To solve this problem, we are developing intelligent software that automatically recognizes sperm. Under the control of the software, the micro-probe can be automatically aligned with the head and neck of the sperm. Moreover, the software can control several micro-probes to work at the same time, thereby increasing the degree of automation of the method and greatly increasing the detection throughput. At present, this work is already in progress, and good progress has been made. Second, due to limited clinical sample resources, we could not obtain a large number of semen samples from infertile men. Therefore, in evaluating the clinical application prospects of this method, we used its ability to detect ROS levels in sperm as the criterion. Although we believe that this method can be used to diagnose oxidative stress infertility, we still need to test more male infertility patients to further prove the clinical value of this method.
In conclusion, we have developed a method that can quantitatively detect fluorescent substances in sperm at the single-cell level and successfully verified the method's strong specificity and high sensitivity by detecting ROS in the sperm of 102 semen samples. This method can accurately determine the level of ROS in sperm, provides a new detection method for assessing sperm quality, and makes a significant contribution to providing evidence for diagnosis and prognosis of male infertility.
This study was approved by the Ethics Committee of the Reproductive Medicine Center, Tongji Medical College, Huazhong University of Science and Technology (approval No. 2021-002). All participants signed informed consent forms, agreeing that their semen samples or data could be used for scientific research.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
This work was supported by the National Natural Science Foundation of China (Nos. 21705053 and 81871732), the Open Foundation of NHC Key Laboratory of Birth Defects Prevention (No. ZD202104) and the Open Foundation of Key Laboratory of Birth Regulation and Control Technology of National Health Commission of China, Maternal Child Health Care Hospital of Shandong Province. We were grateful for the single-cell analysis system provided by Jiangsu Rayme Biotechnology Co., Ltd. and their technical support for the construction of SSRDM in this work.
Supplementary material associated with this article can be found, in the online version, at doi:
F. Zegers-Hochschild, G.D. Adamson, S. Dyer, et al. Hum. Reprod. 32 (2017) 1786–1801. doi: 10.1093/humrep/dex234
M. Vander Borght, C. Wyns, Clin. Biochem. 62 (2018) 2–10. doi: 10.1016/j.clinbiochem.2018.03.012
A. Agarwal, S. Baskaran, N. Parekh, et al., Lancet 397 (2021) 319–333. doi: 10.1016/S0140-6736(20)32667-2
E.A. Taha, A.M. Ez-Aldin, S.K. Sayed, et al., Urology 80 (2012) 822–825. doi: 10.1016/j.urology.2012.07.002
R. Sharma, A. Harlev, A. Agarwal, et al., Eur. Urol. 70 (2016) 635–645. doi: 10.1016/j.eururo.2016.04.010
C. Krausz, A. Riera-Escamilla, Nat. Rev. Urol. 15 (2018) 369–384. doi: 10.1038/s41585-018-0003-3
L.T. Gou, J.Y. Kang, P. Dai, et al., Cell 169 (2017) 1090–1104. doi: 10.1016/j.cell.2017.04.034
A. Agarwal, N. Parekh, M.K. Panner Selvam, et al., World J. Mens. Health 37 (2019) 296–312. doi: 10.5534/wjmh.190055
R.R. Henkel, Asian J. Androl. 13 (2011) 43–52. doi: 10.1038/aja.2010.76
A.D. Bui, R. Sharma, R. Henkel, et al., Andrologia 50 (2018) e13012. doi: 10.1111/and.13012
A. Agarwal, S. Prabakaran, S.S. Allamaneni, Reprod. BioMed. Online 12 (2006) 630–3. doi: 10.1016/S1472-6483(10)61190-X
P. Gogol, B. Szczęśniak-Fabiańczyk, A. Wierzchoś-Hilczer, Reprod. Biol. 9 (2009) 39–49. doi: 10.1016/S1642-431X(12)60093-X
Y. Yumura, A. Iwasaki, K. Saito, et al., Int. J. Urol. 16 (2009) 202–207. doi: 10.1111/j.1442-2042.2008.02213.x
S. Venkatesh, M.B. Shamsi, S. Dudeja, et al., Arch. Gynecol. Obstet. 283 (2011) 121–126. doi: 10.1007/s00404-010-1645-4
R. Mahfouz, R. Sharma, J. Lackner, et al., Fertil. Steril. 92 (2009) 819–827. doi: 10.1016/j.fertnstert.2008.05.087
N. Aziz, J. Novotny, I. Oborna, et al., Fertil. Steril. 94 (2010) 2604–2608. doi: 10.1016/j.fertnstert.2010.03.022
X.T. Zheng, H.B. Yang, C.M. Li, Anal. Chem. 82 (2010) 5082–5087. doi: 10.1021/ac100074n
X.T. Zheng, W. Hu, H. Wang, et al., Biosens. Bioelectron. 26 (2011) 4484–4490. doi: 10.1016/j.bios.2011.05.007
W.H. Organization, WHO laboratory manual for the examination and processing of human semen, 2010.
K. Tremellen, Hum. Reprod. Update 14 (2008) 243–258. doi: 10.1093/humupd/dmn004

Figure 1 (A) The preparation of the capillary with the Ti ring at the microtip. (B) Schematics of the platform for fluorescence detection. (C) FE-SEM image of the optical micro-probe. Scale bar is 1 µm.

Figure 2 (A) Linear relationship of CM-H2DCFDA between the fluorescence intensity and H2O2 concentration (0.05–1 µmol/L). (B) Fluorescence response of CM-H2DCFDA to various common species (20 µmol/L). The red bar shows the fluorescence intensity after the addition of these analytes. (C) Endpoint fluorescence intensity of CM-H2DCFDA oxidized by 2 µmol/L and 20 µmol/L of H2O2 for 30 min in the continuous monitoring mode and endpoint measurement mode. (D, E) A higher fluorescence value (1796) was measured when using the platform to detect bright sperm. (F, G) A lower fluorescence value (26) was measured when using the platform to detect sperm with no visible fluorescence. Scale bar is 10 µm. (H) The result of SSRDM in detecting ROS in sperm of menadione group and control group.

Figure 3 Different methods to show the level of ROS in sperm before and after treatment. (A) Fluorescence microscopy. (B) SSRDM. (C) FCM.

Figure 4 (A) Variability study of storage temperature on detection results of SSRDM. Each column represents the statistical sample population of 20 semen. (B) Variability study of time to be detected on detection results of SSRDM. Each column represents the statistical sample population of 10 semen. **P < 0.01, ***P < 0.001.
Table 1. Different studied semen parameters for non-asthenozoospermia group and asthenozoospermia group.
|
|
 下载: 导出CSV
下载: 导出CSV

 扫一扫看文章
扫一扫看文章

扫一扫关注我们