Figure 1.
Chemical structure of oxaprozin and paeonol
Synthesis and Anti-inflammatory Effects of Oxaprozin-Paeonol Ester
Xuetao Xu , Jie Chen , Zhiqing Lin , Dongli Li , Kun Zhang , Zhaojun Sheng , Shaohua Wang , Shun Zhu , Abdullah M. Asiri

Inflammation, the most widespread disorder, is part of the complex biological response of body tissues to harmful stimuli, including irritants, damaged cells, or patho- gens.[1~3] The chronic inflammation results in the prolonged and oxidative stress, even irreversible damage to tissues.[4, 5] The most common therapeutic drugs for inflammatory symptoms are non-steroidal anti-inflammatory drugs (NSAIDs).[6, 7] Despite their different structure, NSAIDs have a similar action mode by inhibiting the cyclooxygenase (COX) enzyme.[8, 9]
Oxaprozin (a) with a chemical structure of 3-(4, 5-di- phenyl-1, 3-oxazol-2-yl) propanoic acid is one of prominent NSAIDs (Figure 1).[10~14] Oxaprozin exerts its pharmacological effect through the inhibition of COX-dependent inflammation pathway.[15] Moreover, oxaprozin inhibits the NF-κB activation to regulate the inflammatory and immune mediators produced by IκB kinase. But unfortunately, oral medication of oxaprozin potentially induces the gastric perforation, which is caused by the local irritation introduced by the carboxylic acid group of oxaprozin and the ion trapping mechanism from the lumen to mucosa.[16, 17] So far, lots of attempts to mask the carboxylic acid group of NSAIDs are inappropriate, leading to the failure in overcoming NSAIDs based GI complications.
Paeonol (b) is a primary bioactive component of moutan cortex radicis. Numerous researches indicated that paeonol displays excellent biological activity, such as anti-inflam- matory, anti-oxidant, anti-bacterial, anti-diabetic, anti- allergic, and anti-angiogenic.[18~20] Also, paeonol has been used to treat skin pruritus, rheumatoid arthritis, and pain in China.[21] The anti-inflammatory of paeonol is contributed to its regulation on reactive oxygen, iNOS, COX-2, and proinflammatory cytokines including TNF-α and IL-1β.[22] In signal molecule level, some reports have shown that paeonol achieves its antioxidant and anti-inflammatory activity through inhibition or blocking the MAPK, ERK, and p38 signaling pathways.[23, 24]
The structural modification of the carboxyl group of NSAIDs is an effective way to reduce the irritating side effects of GI perforation.[25] Also, the introduction of antioxidant groups might enhance anti-inflammatory effects of maternal skeleton.[26] To effectively manage inflammatory diseases and overcome the oxaprozin based GI complications, there is a urgent need to intervene an anti-inflamma- tory and anti-oxidant group. Hence, the synthesis of oxaprozin-paeonol ester (OPE) exploiting the anti-inflammatory and anti-oxidant capacity of paeonol to mask the carboxylic acid group of oxaprozin was reported.
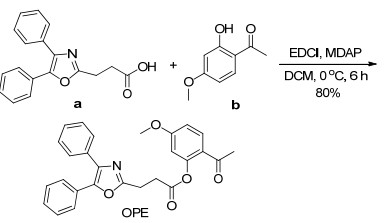
As shown in Scheme 1, OPE was prepared by the reaction between oxaprozin and paeonol in yield of 80%, and used for the following biological experiments. Next, the biological properties of oxaprozin, paeonol and OPE were evaluated.
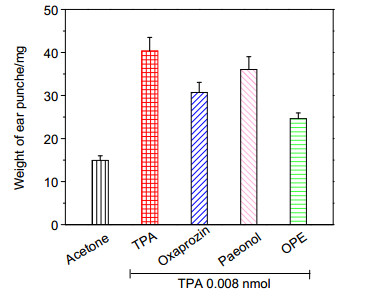
In recent years, TPA-induced ear edema has been developed into a mature animal model of inflammation due to its advantages of simple operation, stable model, and often used to evaluate the anti-inflammatory activity of compound.[27~29] So the effect of OPE on TPA-induced ear edema was investigated. According to our previous publications, the concentration of TPA was selected as 0.008 nmol•L-1, and compound concentration was selected as 0.75 μmol•L-1.[30, 31] As shown in Figure 2, topical treatment of TPA alone led to a significant increase in the weight of ear punches from 14.9 mg to 40.4 mg, which verified that TPA could stimulate the progress of inflammatory. While pretreatment with oxaprozin and paeonol, OPE could obviously reduce the weight of ear punches compared to TPA treatment alone. And the inhibitory effect of OPE on TPA-induced ear edema model was 61.8%, which was about 2 times higher than that of oxaprozin and 4 times than that of paeonol. These results indicate that OPE potential plays a synergy of oxaprozin and paeonol on treat TPA-induced inflammatory.
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05
When stimulated with TPA, the ear skin appears a significant increase of skin thickening, which is linked with the edema, proliferation of epidermal keratinocytes, and increase of vascular permeability.[32] The disorders of inflammatory tissue can be evaluated by its histological appearance. In control tissues only treated with acetone (Figure 3a), there was a normal performance in epidermal layer without any significant lesion. When stimulated with TPA, the ear occurred obviously inflammation leading to epidermal hyperplasia, hyperkeratosis, and leukocyte infiltration of tissue (Figure 3b), which is consistent with the results of previous report.[30] It is amazing that topical pretreatment with oxaprozin, paeonol, and OPE obviously prevented the feature of inflammatory responses (Figures 3c~3e). Those results revealed that OPE could effectively relieve TPA-induced inflammatory.

Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×
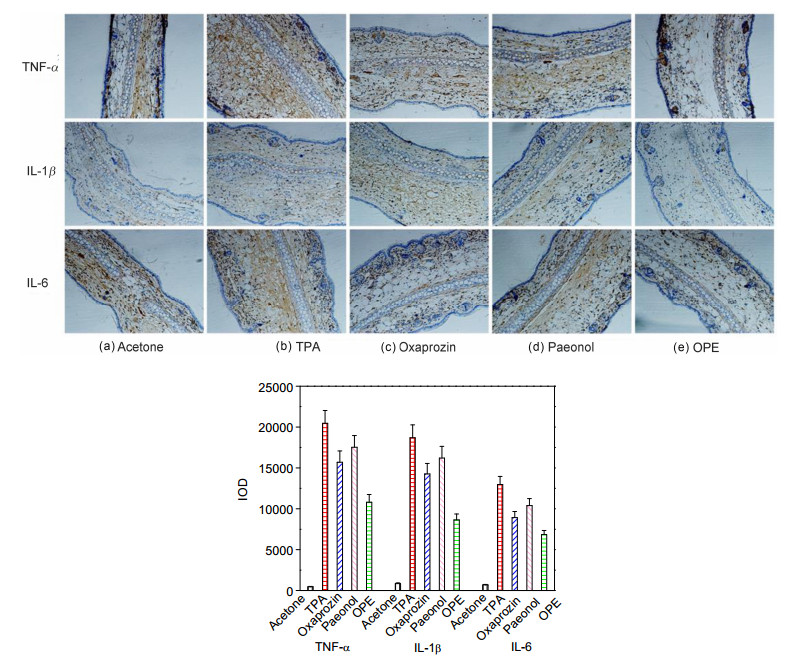
Cytokines are protein molecules, which help to regulate the immune response of body against infection and trauma.[33, 34] After been stimulated, cells produce a variety of proinflammatory cytokines including TNF-α, IL-1β, and IL-6 to accelerate the process of inflammatory.[34, 35] Then, we investigated whether or not OPE has effect on TPA-induced TNF-α, IL-1β, and IL-6. Wu et al.[25] verified that TPA induced the secretion of inflammatory factors. As shown in Figure 4b, TPA stimulation resulted in the obvious increase on the expression of TNF-α, IL-1β, and IL-6 compared with control (Figure 4a). However, the topical pretreatment with oxaprozin, paeonol, and OPE could markedly reduce the expression of TPA-induced TNF-a, IL-1β, and IL-6 (Figures 4c~4e). Also the effects of OPE on TPA-induced TNF-α, IL-1β, and IL-6 were higher than those of oxaprozin and paeonol. These results also confirmed that inflammatory process was closely related to the expression of TNF-α, IL-1β, and IL-6.
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×
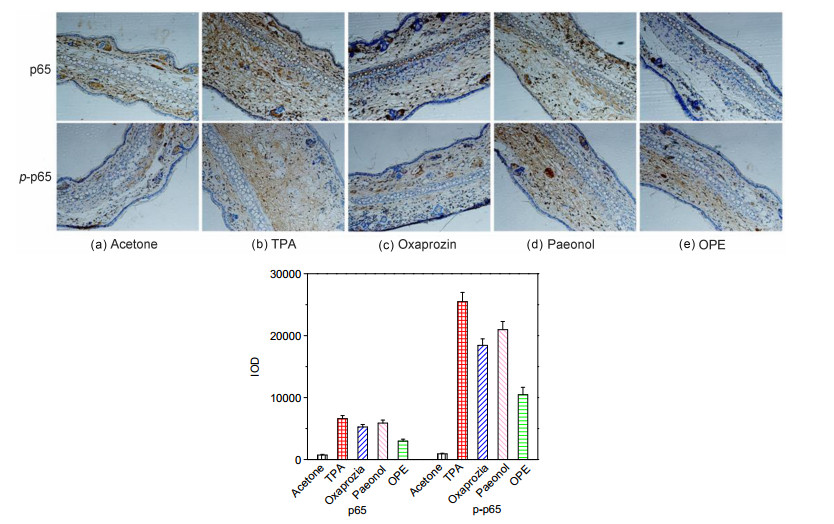
Nuclear factor κB (NF-κB) consist p50, p52, p65, Rel, and RelB is a nuclear transcription factor that regulates expression of a large number of genes. They are critical for the regulation of apoptosis, viral replication, tumorigenesis, inflammation, and various autoimmune diseases.[36, 37] Cytokines including TNF-α, IL-1β, and IL-6 involved in inflammation are regulated by NF-κB.[38, 39] Herein, it is very important to evaluate how OPE effects the TPA-induced NF-κB activation. Here, the effect of OPE on p65 was investigated. After TPA stimulated (Figure 5b), p65 was evoked nuclear translocation to the nucleus indicating an obviously increased expression. Figures 5c~5e also show that topical pretreatment with oxaprozin, paeonol, and OPE could strongly block the expression of TPA-induced p65. Moreover, topical pretreatment with oxaprozin, paeonol, and OPE also markedly decrease the expression of TPA-induced phosphor-p65, which contributes to its transcriptional activity (Figures 5c~5e). Thence, the anti-inflammation effect of OPE is linked to its inhibition ability on NF-κB activation.
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×
It has been demonstrated that phosphorylation of IκB proteins including IκBα is essential for NF-κB activation. The degradation of IκB arouses NF-κB to translocate into nucleus.[40] The IκB kinase (IKK) plays key roles in phosphorylating IκBα[41]. And IKK has been reported to highly relate with the NF-κB activation.[42] Then the effect of OPE on TPA-induced IKK was investigated. As described in Figure 6b, TPA stimulation resulted in the degradation of IκBα accompanies with its phosphorylation. The topical pretreatment with oxaprozin, paeonol, and OPE markedly suppressed the phosphorylation of IκBα (Figures 6c~6e). Moreover, topical pretreatment with oxaprozin, paeonol, and OPE obviously reduced the TPA-induced IKK activity (Figures 6a~6e). The results suggested that OPE inhibited activation of NF-κB by blocking IKK activities.
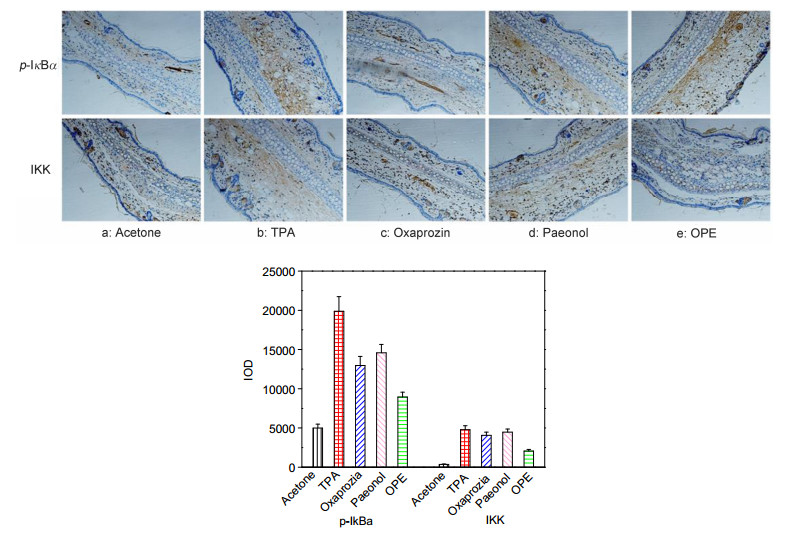
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×
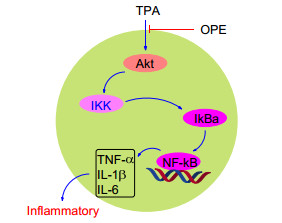
Besides IKK, NF-κB molecule is regulated by Akt signal pathway. Activated Akt signal is also involved in the phosphorylation and degradation of IκB, resulting in the NF-κB activation.[43] In addition, Akt signal pathway is involved in the mediation of pro-inflammatory cytokines including TNF-α, IL, and IFN.[44~46] So the effect of OPE on Akt signal pathway was investigated. As illustrated in Figure 7, TPA stimulation caused significant increases on expressions and phosphorylation of Akt. And topical pre- treatment with oxaprozin, paeonol, and OPE significantly inhibited the TPA-induced Akt activity (Figures 7c~7e). All the results revealed that OPE exerted its anti-inflam- matory through down-regulating the NFκB activation by blocking Akt/IKK activities (Figure 8).
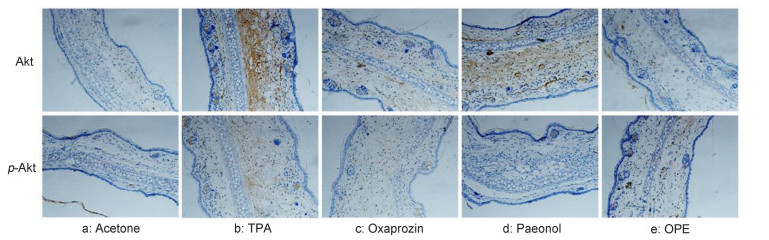
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×
Inspired by paeonol, a natural antioxidants and antiulcerogenic, OPE had been designed and synthesized to avoid the GI complications of oxaprozin. In TPA-induced mouse ear edema model, OPE showed more beneficial effects on anti-inflammatory than that of oxaprozin or paeonol, including swelling, histological change, and release of proinflammatory cytokines. In addition, this study also revealed that the anti-inflammatory of OPE was associated with its ability to down-regulate activation of NF-κB by blocking Akt/IKK activities. Currently, the development of more potent lead compounds is ongoing in the same lab.
Oxaprozin and paeonol were obtained from Shanghai Aladdin Bio-Chem Technology Co., LTD (China). 12-O- Tetradecanoylphorbol 13-acetate (TPA) was purchased from Sigma Chemical Co. (USA). 1H NMR and 13C NMR spectra of OPE were recorded on a Bruker AM-600 NMR spectrometer (USA) in CDCl3. Elemental analysis was conducted with a Series II 2400 elemental analyzer (USA). Melting point was measured with automatic melting point instrument (China). IR was recorded using a Shimadzu fourier transform infrared spectrometer (Japan). TNF-a, IL-1β, IL-6, anti-rabbit, anti-mouse horseradish peroxidase (HRP)-conjugated secondary antibodies, anti-Ser536 p65, antiphospho-Ser536 p65 antibodies, antiphospho-Ser32 IkB-α, anti-IKK, anti-Ser473 Akt, antiphospho-Ser473 Akt were obtained from Beyotime Biotechnology Co. (China). Other chemicals used were obtained form available commercially.
Oxaprozin (146.8 mg, 0.5 mmol), paeonol (84.2 mg, 0.5 mmol), EDCI (144.5 mg, 0.75 mmol) and DMAP (61.4 mg, 0.5 mmol) were mixed in dichloromethane (DCM, 5 mL) at 0 ℃. The mixture was stirred for 6 h at 0 ℃, then quenched with water. The aqueous layer was extracted three times with EtOAc and the combined organic layers were washed with brine, dried over sodium sulfate, and evaporated to dryness and purified by column chromatography to afford OPE as a white solid (182.4 mg, 80%). m.p. 114~115.5 ℃; 1H NMR (400 MHz, CDCl3) δ: 7.75 (d, J=8.8 Hz, 1H), 7.61~7.54 (m, 2H), 7.55~7.49 (m, 2H), 7.33~7.17 (m, 6H), 6.74 (dd, J=8.8, 2.5 Hz, 1H), 6.54 (d, J=2.5 Hz, 1H), 3.67 (s, 3H), 3.27 (t, J=6.9 Hz, 2H), 3.18 (t, J=6.9 Hz, 2H), 2.44 (s, 3H); 13C NMR (101 MHz, CDCl3) δ: 195.63, 170.63, 163.79, 161.62, 151.42, 145.56, 135.15, 132.48, 128.98, 128.64, 128.55, 128.47, 128.06, 127.93, 126.54, 122.86, 112.08, 109.06, 55.62, 31.33, 29.70, 29.06; IR (KBr) ν: 3065, 2915, 2848, 1756, 1576, 1496, 1425, 1201, 1139, 914, 822, 765, 693 cm-1. Anal. calcd for C27H23NO5: C 73.46, H5.25, N 3.17; found C 73.38, H 5.26, N 3.12.
Female ICR mice at 6 weeks old were supplied from Guangdong Medical Laboratory Animal Center (China). All mices were housed in condition of (25±1) ℃ at 50% relative humidity, fed with food and water ad libitum. This experiments were maintained in accordance with the guidelines of Guangdong Medical Laboratory Animal Center, and approved by the institutional ethical committee of Wuyi University.
Oxaprozin, paeonol, OPE, and TPA were dissolved in acetone. Mice were randomly divided into 5 groups, and each group had four mice. For TPA-induced mouse ear edema model, the right ears of mice were topical treated with acetone, oxaprozin, paeonol, and OPE respectively, and stimulated with TPA after 30min. The mice un-stimulated with TPA were set as control. All mice were euthanized after 6 h, and the ear punches of 9 mm diameter from mice right ears were taken and weighed. Then inhibitory effe- cts=[(Wa-Wb)/(Wa-Wc)]×100%. Where, Wa is the weight of ear treated with TPA alone, Wb is the weight of ear treated with TPA + test compound, Wc is the weight of ear treated with acetone alone.
Mice ear punches were selected and fixed in 10% formalin. After decalcified in EDTA buffer and subjected dehydration, ear punches were embedded into paraffin. The slice of 4 μm was serially sectioned, and stained with routinely H & E staining. Then the histological changes of mice ear were observed under a microscope.
The TNF-α, IL-1β, and IL-6 levels were determined as described previously.[47, 48] After deparaffinized treatment, the ear slices were incubated in H2O2 (1.2%). Ear slices then were treated with the primary antibody of proliferating cell nuclear antigen (1:100) overnight at 4 ℃. After washed, the ear slices were incubated into biotin-conju- gated horseradish peroxidase antibody (1:200) for 1 h at 25 ℃. Then the peroxidase was detected with 3, 3-dia- minobenzidine tetrahydrochloride reactions, resulting to a brown label in ear tissue. For each ear slice, the positive staining cell numbers were counted in randomly five different fields.
The effects of OPE on the NF-κB, Akt, IKK signal pathway were measured by immunohistochemistry analysis as described in our previous work.[49, 50] Mice ears were selected, fixed, and embedded in paraffin. The sectioned ear slices of 4 μm were stained with routinely staining method, and the positive staining cell numbers were counted in randomly five different fields.
The assays of IL-1β, IL-6, TNF-α, p65, p-p65, p-IκBα, IKK, Akt, and p-Akt were detected using integrated optical density (IOD) following semi-quantitative scoring sys- tem[51]. The staining intensity was scored as follows: 0, no staining; 1+, faint; 2+, moderate; 3+, strong. The staining extent was graded as follows: 0, no staining; 1+, ≤25% of cells positive; 2+, 26%~50% of cells positive; 3+, ≥51% of cells positive.[52]
All results are presented as mean±SE. Comparison between groups was calculated with one-way analysis of variance (ANOVA) followed by Dunnett's t-test. P < 0.05 was considered indicative of significance.
Talaat, R.; El-Sayed, W.; Agwa, H. S.; Gamal-Eldeen, A. M.; Moawia, S.; Zahran, M. A. H. Chem.-Biol. Interact. 2015, 238, 74. doi: 10.1016/j.cbi.2015.05.017
McInnes, I. B.; Schett, G. Nat. Rev. Immunol. 2007, 7, 429. doi: 10.1038/nri2094
Shin, J. S.; Choi, H. E.; Kim, S. D.; Lee, Y. S.; Cho, Y. W.; Lee, K. T. Chem. Biol. Interact. 2014, 224, 68. doi: 10.1016/j.cbi.2014.10.004
Wu, J.; Chu, C. C. J. Mater. Chem. B 2013, 1, 353. doi: 10.1039/C2TB00070A
Wu, J.; Chu, C. C. Acta Biomater. 2012, 8, 4314. doi: 10.1016/j.actbio.2012.07.027
Rao, P. P. N.; Kabir, S. N; Mohamed, T. Pharmaceuticals 2010, 3, 1530.
Rainsford, K. D.; Whitehouse, M. W. Inflammopharmacology 2006, 14, 150. doi: 10.1007/s10787-006-1389-8
Robak, P.; Smolewski, P.; Robak, T. Leuk Lymphoma 2008, 49, 1452. doi: 10.1080/10428190802108854
Macario, A.; Lipman, A. G. Pain Med. 2001, 2, 336. doi: 10.1046/j.1526-4637.2001.01043.x
al-Faks, M. A.; Pugh, M. C. Orthop. Rev. 1995, 21, 558.
Bozic, B. D.; Rogan, J. R.; Poleti, D. D.; Trisovic, N. P.; Uscumlic, G. S. Chem. Pharm. Bull. 2012, 60, 865. doi: 10.1248/cpb.c12-00185
Rainsford, K. D.; Omar, H.; Ashraf, A.; Hewson, A. T. R.; Bunning, A. D.; Rishiraj, R.; Shepherd, P.; Seabrook, R. W. Inflammopharmacology 2002, 10, 185. doi: 10.1163/156856002321168204
Lopes-de-Araújo, J.; Neves, A. R.; Gouveia, V. M.; Moura, C. C.; Nunes, C.; Reis, S. Pharm. Res. 2016, 33, 301. doi: 10.1007/s11095-015-1788-x
Peesa, J. P.; Atmakuri, L. R.; Yalavarthi, P. R.; Venkata, B. R. M.; Rasheed, A.; Pachava, V. Arch. Pharm. Chem. Life Sci. 2017, 351, e1700256.
Dallegri, F.; Bertolotto, M.; Ottonello, L. Exp. Opin. Ther. 2005, 1, 777.
Peesa, J. P.; Yalavarthi, P. R.; Rasheed, A.; Mandava, V. B. J. Acute Dis. 2016, 1, 364.
Bandgar, B. P.; Sarangdhar, R. J.; Viswakarma, S.; Ahamed, F. A. J. Med. Chem., 2011, 1, 1191.
Chou, T. C. Br. J. Pharmacol. 2003, 139, 1146. doi: 10.1038/sj.bjp.0705360
Huang, T. J.; Chuang, H.; Liang, Y. C.; Lin, H. H.; Horng, J. C.; Kuo, Y. C.; Chen, C. W.; Tsai, F. Y.; Yen, S. C.; Chou, S. C.; Hsu, M. H. Eur. J. Med. Chem. 2015, 90, 428. doi: 10.1016/j.ejmech.2014.11.050
Nizamutdinova, I. T.; Jin, Y. C.; Kim, J. S.; Yean, M. H.; Kang, S. S.; Kim, Y. S.; Lee, J. H.; Seo, H. G.; Kim, H. J.; Chang, K. C. Planta Med. 2008, 74, 8.
Huang, L.; Zhang, B.; Yang, Y.; Gong, X.; Chen, Z.; Wang, Z.; Zhang, P.; Zhang, Q. Bioorg. Med. Chem. Lett. 2016, 26, 5218. doi: 10.1016/j.bmcl.2016.09.060
Zhang, H.; Chen, S.; Deng, X.; Yang, X.; Huang, X. Diabetes Res. Clin. Pract. 2006, 74, 194. doi: 10.1016/j.diabres.2006.04.003
Nizamutdinova, I. T.; Oh, H. M.; Min, Y. N.; Park, S. H.; Lee, M. J.; Kim, J. S.; Yean, M. H.; Kang, S. S.; Kim, Y. S.; Chang, K. C.; Kim, H. J. Int. Immunopharmacol. 2007, 7, 343. doi: 10.1016/j.intimp.2006.11.004
Jin, X.; Wang, J.; Xia, Z. M.; Shang, C. H.; Chao, Q. L.; Fan, H. Y.; Chen, D. Q.; Qiu, F.; Zhao, F. Inflammation 2016, 39, 434. doi: 10.1007/s10753-015-0265-3
Wu, P. P.; He, H.; Hong, W. D.; Wu, T.; Huang, G.; Zhong, Y.; Tu B.; Gao, M.; Zhou, J.; Zhao, S.; Li, D.; Xu, X. T.; Sheng, Z.; Ward, S. A.; O'Neill, P. M.; Zhang, K. Infect. Drug Resist. 2018, 11, 1945. doi: 10.2147/IDR.S176390
Xu, L.; Mou, X. Q.; Chen, Z. M.; Wang, S. H. Chem. Commun. 2014, 50, 10676. doi: 10.1039/C4CC04640D
Hernández, V.; Má ez, S.; Recio, M. C.; Giner, R. M.; Ríos, J. L. Eur. J. Pharm. Sci., 2005, 26, 162. doi: 10.1016/j.ejps.2005.05.007
Mehrotra, A.; Shanbhag, R.; Chamallamudi, M. R.; Singh, V. P.; Mudgal, J. Eur. J. Pharm. 2011, 666, 80. doi: 10.1016/j.ejphar.2011.05.039
Hernández, I.; Márquez, L.; Martínez, I.; Dieguez, R.; Delporte, C.; Prieto, S.; Molina-Torres, J.; Garrido, G. J. Ethnopharmacol. 2009, 124, 649. doi: 10.1016/j.jep.2009.04.060
Xu, X. T.; Mou, X. Q.; Xi, Q. M.; Liu, W. T.; Liu, W. F.; Sheng, Z. J.; Zheng, X.; Zhang, K.; Du, Z. Y.; Zhao, S. Q.; Wang, S. H. Bioorg. Med. Chem. Lett. 2016, 26, 5334. doi: 10.1016/j.bmcl.2016.09.034
Xu, X. T.; Huang, D. Y.; Liu, W. F.; Sheng, Z. J.; Liang, K. Y.; Li, D. L.; Zhao, D.; Ma, Y.; Zhang, K.; Hayat, T.; Alharbif, N. S.; Li, W. K. RSC Adv., 2017, 7, 34699. doi: 10.1039/C7RA01111C
Rao, T. S.; Currie, J. L.; Shaffer, A. F.; Isakson, P. C. Inflammation 1993, 17, 723. doi: 10.1007/BF00920477
Hauser, C.; Dayer, J. M.; Jaunin, F.; de Rochemonteix, B.; Saurat, J. H. Cell. Immunol. 1986, 100, 89. doi: 10.1016/0008-8749(86)90009-2
Kock, A.; Schwarz, T.; Kirnbauer, R.; Urbanski, A.; Perry, P.; Ansel, J. C.; Luger, T. A. J. Exp. Med. 1990, 172, 1609. doi: 10.1084/jem.172.6.1609
Kupper, T. S.; Ballard, D. W.; Chua, A. O.; McGuire, J. S.; Flood, P. M.; Horowitz, M. C.; Langdon, R.; Lightfoot, L.; Gubler, U. J. Exp. Med. 1986, 164, 2095. doi: 10.1084/jem.164.6.2095
Singh, S.; Aggarwal, B. B. J. Biol. Chem. 1995, 270, 10631. doi: 10.1074/jbc.270.18.10631
Han, S. S.; Keum, Y. S.; Seo, H. J.; Chun, K. S.; Lee, S. S.; Surh, Y. J. Cancer Lett. 2001, 164, 119. doi: 10.1016/S0304-3835(01)00378-0
Kim, S. O.; Kundu, J. K.; Shin, Y. K.; Park, J. H.; Cho, M. H.; Kim, T. Y.; Surh, Y. J. Oncogene 2005, 24, 2558. doi: 10.1038/sj.onc.1208446
Zandi, E.; Rothwarf, D. M.; Delhase, M.; Hayakawa, M.; Karin, M. Cell 1997, 91, 243. doi: 10.1016/S0092-8674(00)80406-7
Li, Z. W.; Chu, W.; Hu, Y.; Delhase, M.; Deerinck, T.; Ellisman, M.; Johnson, R.; Karin, M. J. Exp. Med. 1999, 189, 1839. doi: 10.1084/jem.189.11.1839
Karin, M.; Delhase, M. Semin. Immunol. 2000, 12, 85. doi: 10.1006/smim.2000.0210
Carpenter, C. L.; Cantley, L. C. Curr. Opin. Cell Biol. 1996, 8, 153. doi: 10.1016/S0955-0674(96)80060-3
Karin, M. Oncogene 1999, 18, 6867. doi: 10.1038/sj.onc.1203219
Shimamura, H.; Terada, Y.; Okado, T.; Hiroyuki, T.; Inoshita, S.; Sadak, S. J. Am. Soc. Nephrol. 2003, 14, 1427. doi: 10.1097/01.ASN.0000066140.99610.32
Selvaraj, S. K.; Giri, R. K.; Perelman, N.; Johnson, C.; Malik, P.; Kalra, V. K. Blood 2003, 102, 1515. doi: 10.1182/blood-2002-11-3423
Hatcher, H.; Planalp, R.; Cho, J.; Torti, F. M.; Torti, S. V. Cell. Mol. Life Sci. 2008, 65, 1631. doi: 10.1007/s00018-008-7452-4
V. Stefano, D. M. Paolo, S. Rossana and L. Luisa, J. Drugs Dermatol. 2009, 8, 537.
Liu, W. F.; Li, Y. L.; Zhang, K.; Du, Z. Y. Food Funct. 2015, 6, 3712. doi: 10.1039/C5FO00899A
Liu, W. F.; Li, Y. L.; Zheng, X.; Zhang, K.; Du, Z. Med. Chem. Commun. 2015, 6, 1605. doi: 10.1039/C5MD00227C
Liu, W. F.; Li, Y. L.; Yue, Y.; Zhang, K.; Chen, Q.; Wang, H. Q.; Lu, Y. J.; Huang, M. T.; Zheng, X.; Du, Z. Y. Bioorg. Med. Chem. Lett. 2015, 25, 3044. doi: 10.1016/j.bmcl.2015.04.077
Kraan, M. C.; Haringman, J. J.; Ahern, M. J.; Breedveld, F. C.; Smith, M. D.; Tak, P. P. Rheumatology 2000, 39, 43.
Ouyang, N.; Williams, J. L.; Tsioulias, G. J.; Gao, J. J.; Iatropoulos, M. J.; Kopelovich, L.; Kashfi, K.; Rigas, B. Cancer Res. 2006, 66, 4503. doi: 10.1158/0008-5472.CAN-05-3118

Figure 2 Effect of oxaprozin, paeonol, OPE on TPA-induced ear edema
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05

Figure 3 Effect of oxaprozin, paeonol, OPE on TPA-induced histological changes of ear edema (H & E staining)
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×

Figure 4 Effect of oxaprozin, paeonol, OPE on TPA-induced TNF-α, IL-1β, and IL-6
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×

Figure 5 Effect of oxaprozin, paeonol, OPE on TPA-induced NF-κB activation
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×

Figure 6 Effect of oxaprozin, paeonol, OPE on TPA-induced IKK
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×

Figure 7 Effect of oxaprozin, paeonol, OPE on TPA-induced Akt
Data are presented as mean±SE (n=4). Compared to TPA alone, *P < 0.05. Magnification 200×

 扫一扫看文章
扫一扫看文章

扫一扫关注我们
 下载:
下载:

 下载:
下载:

